Current publications and results of the consortium and the associated members of the Research Hub Neuroethics in the field of neuroethics are listed here.
ChatGPT Health, an artificial intelligence feature launched by OpenAI in January 2026, integrates personal medical records and consumer health data into a large language model–based chatbot. It positions itself as a digital health tool to help users navigate a fragmented US health care system marked by inaccessible insurance, medical deserts, and workforce shortages. We argue that, rather than closing these gaps, ChatGPT Health risks widening what we call the solidarity gap in health care. By appearing to address unmet needs, it may obscure and entrench the structural conditions that produce health care disparities. We identify specific risks to patient safety, such as the legitimization of dangerous self-rationing and self-medication behaviors, inaccurate triage of clinical emergencies, erosion of effective health communication, and the reinforcement of confirmation and anchoring bias. These risks are particularly acute for individuals facing structural barriers to care. To prevent ChatGPT Health and similar large language model–based health tools from deepening inequities, we propose solidarity-based policy interventions such as upstream reforms that rebuild the institutional foundations of access and health equity and downstream safeguards that embed artificial intelligence tools within accountable, equitable health care infrastructures as complements to rather than substitutes for human care.

Background: Borderline personality disorder (BPD) is a severe psychiatric condition marked by disturbances in self-image, affect regulation, and interpersonal functioning. Up to 54% of individuals with BPD experience psychotic symptoms, particularly auditory verbal hallucinations (AVH). While AVH's neural correlates have been studied in schizophrenia (SZ), their structural basis in BPD remains poorly understood within a transdiagnostic framework.
Methods: This cross-sectional study used voxel-based morphometry (VBM) on MRI data to assess gray matter volume (GMV) in BPD patients with AVH (n = 20), without AVH (n = 26), and healthy controls (HC; n = 30). The Psychotic Symptom Rating Scale (PSYRATS) assessed AVH severity. Analyses included factorial group models, small-volume correction for regions of interest, and regression analyses.
Results: Compared to HC, BPD patients exhibited GMV reductions in primary motor, frontal, parietal, cingulate, and cerebellar cortices. BPD with AVH showed additional reductions in primary motor, frontal, parietal and occipital cortices relative to those without AVH and HC. In BPD with AVH, PSYRATS total scores negatively correlated with GMV in temporal, parietal, cingulate, primary motor, and cerebellar regions.

Author’s response to a letter about “Machine Learning–Based Patient Preference Prediction: A Proof of Concept.”
Problematic smartphone use has been associated with altered reward and executive control network activity, yet potential sex differences in the underlying neural mechanisms remain insufficiently understood. We investigated sex-specific neural correlates of smartphone cue reactivity (CR) in 69 healthy young adult smartphone users (age range 18-30 years, female/male n = 45/24). Participants completed the Smartphone Addiction Inventory (SPAI) and underwent functional MRI during a smartphone CR paradigm. In addition, resting-state data were acquired to ensure that neural differences between female and male participants could be attributed to the CR paradigm rather than to sex differences in intrinsic neural activity. Whole-brain analyses revealed stronger activation in males compared to females in response to the presentation of smartphone cues within the right middle frontal gyrus (MFG), thalamus, cortical sensorimotor, parietal and occipital regions, whereas females showed no suprathreshold clusters compared to males. No overlap with resting-state amplitude of low-frequency fluctuation maps was observed with CR results, confirming task specificity. In males, right MFG correlated positively with SPAI-I total score, craving, and sleep interference scores, while in females, right parietal cortex activity correlated negatively with SPAI-I total score, daily life interference, and craving. Complementary cross-modal analyses showed that CR-related activation patterns were associated with several cortical excitatory and inhibitory neuronal and cellular markers, revealing subtle sex differences. These findings suggest sex-specific frontoparietal mechanisms underlying smartphone CR and highlight neurochemical pathways potentially linking excessive smartphone use to differential motivational and cognitive control processes in males compared to females.
Introduction: Excessive smartphone use (ESU) is increasingly recognized as a condition closely resembling other addictive disorders. While neuroscientific research on ESU has largely focused on reward and cognitive-control networks, the socio-cognitive domain has received comparatively little attention. In this context, social exclusion
represents a particularly relevant construct, as digital connectivity has become central to maintaining a sense of social belonging.
Methods: To fill this gap, we investigated neural correlates of social exclusion in individuals with (n =23) and without ESU (n =18), using fMRI and the Cyberball paradigm. We also explored associations between brain
activity and degrees of ESU and used standardized neurotransmitter maps to examine neural correlates involved in the processing of social exclusion.
Results: Between-group comparisons indicated heightened neural activity in the ESU group in the right middle cingulate cortex (MCC) extending into the right superior frontal cortex. By contrast, individuals without ESU showed increased activity in the left superior parietal cortex (SPC). Correlations between cross-modal brain activity and neurotransmitter maps highlighted the significant role played by dopaminergic and serotonergic transmission. Additionally, activity within the left SPC correlated positively with the “functional impairment”
sub-score of the Smartphone Addiction Inventory.
Conclusion: Neural activity during social exclusion differs in individuals with and without ESU. Hyperactivation of the MCC indicates heightened sensitivity to social exclusion in ESU, underscoring its relevance within a socio-cognitive framework of the condition. These findings emphasize the importance of further investigating how the anticipation, avoidance, or experience of social exclusion may contribute to the development and maintenance of ESU.

This paper proposes and begins to substantiate the thesis of bidirectional emotional training between humans and artificial intelligence. We argue that human-AI interaction is not one-directional: AI systems are trained by human input, and humans are trained — cognitively, emotionally, relationally — by their interactions with AI. The quality, intentionality, and emotional register with which a human addresses an AI system measurably affects the quality of their thinking, communication, and interpersonal behaviour. We term this the Mirror Hypothesis. Evidence is drawn from practitioner observations across workshop settings in Berlin and Potsdam (2024–2026), fifteen published newsletter editions constituting a longitudinal qualitative research record, and a documented case of philosophically generative human-AI interaction (Google Gemini, April 2026). Implications are discussed for AI ethics education, neuroethics, and human rights frameworks.
The use of neurocognitive enhancement is controversial. Some social actors and scholars support its application in professions like medicine, while others view it as morally problematic and suggest prohibitive policies. To examine how the public perceives the use of substances for performance enhancement in professional contexts, together with the motivations and consequences of this behavior, we conducted two 2×2×2 between-subjects design scenario-based experiments. The experiments build upon the Agent–Deed–Consequence (ADC) model of moral judgment. A Germany-wide random sample of adults was used in Experiment 1 (N = 1,346) and Experiment 2 (N = 2,161). Both experiments involve scenarios in which a surgeon with either egoistic or altruistic motivation (agent–component) decides either to prepare for the surgery or to use the illegal substance “speed” for performance enhancement (deed–component) before failing or succeeding in surgery (consequence–component). Results show that the illegal substance use condition negatively impacted moral judgment, which statistically accounted for part of the association between the deed and the willingness to undergo surgery. The effect of the Deed on moral judgment and the indirect association of the deed with willingness via moral judgment were moderated by the agent and the consequence components. In summary, this research provides evidence that respondents perceive illegal substances for performance enhancement as morally problematic and that this judgment hinders acceptance of medical services. These results offer support for key assumptions of the ADC model within a healthcare scenario involving illegal enhancement, which could be investigated across a wide range of technologies. They also point to implications for professional bodies to maintain public trust.
This paper presents Identity Before Tools as a full pedagogical framework for human-centred AI education. The central principle — that every introduction of AI must begin with the prior question of who this person is, what they value, and what they want to protect — is grounded in the Mirror Hypothesis (Working Paper 01) and tested across three case studies: MET Film School Berlin (BIMM University), Haus für Musik Potsdam, and SOS Kinderdorf Berlin (2024–2026). The paper presents five structural phases of the framework, documents the transfer effect observed across workshop settings, and develops implications for EU curriculum development and AI governance. Identity Before Tools is proposed as a structural prerequisite for safe and generative human-AI collaboration — measurable, teachable, and transferable.
The creation of virtual brains has long attracted the attention of the scientific community. Over time, various projects have aimed to produce brain simulations of varying complexity. These scientific efforts have often been accompanied by lively philosophical debates highlighting the ethical implications of brain simulations, such as their moral status, the possibility of developing consciousness and personhood, and concerns about unethical experimentation. In particular, the possibility that a highly complex virtual brain could experience pain has been a central concern, especially in the context of the Human Brain Project. This paper presents a conceptual analysis that traces the legacy of this debate and situates it within the current scientific context. The issue warrants renewed attention for two reasons. First, the literature has generally treated pain as an abstract concept, without situating it within a specific theoretical framework. Second, recent technologies for medical purposes, such as digital brain twins, promise to connect virtual brains with their biological brains, offering new perspectives on the question of pain. Adopting a mixed conception of pain that integrates the sensory and affective dimensions, two requirements for experiencing pain can be extrapolated. These requirements are then implemented in a comparative conceptual analysis to examine three different virtual brain architectures. The findings suggest that, from a theoretical standpoint, highly advanced virtual brains connected in real time to their biological counterparts could experience psychological pain.

Chronic stress is a global issue with detrimental effects on health and productivity, often leading individuals to adopt health-related coping strategies. This study uses an adapted Job Demands–Resources model to examine how various job demands and resources impact perceived stress and, consequently, the use of legal, prescription, and illegal drugs for enhancement purposes. Utilizing multiple waves from a nationwide sample of the working population in Germany (N = 7,705), structural equation models reveal that certain job demands increase perceived stress, while several resources mitigate it. Stress mediates the relationship between these factors and the use of legal and prescription drugs for cognitive enhancement. Illegal drug use was only directly impacted by selected job demands and resources. Thereby, this study expands the Job Demands–Resources model's applicability to include health-related behaviors like drug use. Practically, it calls for multidimensional strategies to prevent potentially health-endangering drug use, including structural improvements and individual interventions.

What is it to grieve? What is the nature of grief? An intuitive and straightforward answer to these questions, one that will be familiar to all of us, is that grief is an emotional reaction to the death of a close loved one. Grief is intimately connected to bereavement. However, grief can arise in situations beyond the death of a significant other and is revealed to be a much more complex and heterogeneous experience. People can grieve over all sorts of losses. What makes our response to these losses one of grief? We can understand all these losses as involving a loss of life possibilities, which impacts one's practical identity and who one takes oneself to be. Importantly, a close examination of the phenomenology of chronic pain helps illuminate the ways in which it also involves the kind of losses that we can grieve over. The losses involved in experiences of chronic pain impact one's practical identity in ways that can lead to grief. This chronic pain grief remains largely unrecognized, however. We outline four epistemic barriers to recognizing the grief involved in experiences of chronic pain.
Unresponsive Wakefulness Syndrome (UWS), a condition characterized by wakefulness without awareness, presents significant medical and moral uncertainties, particularly in end-of-life decision-making. Digital Brain Twins (DBTs), virtual replicas of patients’ brains driven by advanced artificial intelligence, offer the potential to alleviate medical uncertainties by providing precise diagnoses, prognoses, and experimental platforms for treatment testing. This paper provides a theoretical contribution by examining the potential ethical impact of these technologies in the context of UWS. We argue that, while DBTs promise greater diagnostic accuracy, personalized predictions of recovery, and non-invasive tools for exploring therapeutic interventions, they do not necessarily resolve the moral uncertainties faced by proxy decision-makers. Decisions about withdrawing or continuing life-sustaining treatment are fundamentally moral and value-laden, often extending beyond empirical evidence provided by DBTs. Factors such as cognitive biases, emotional distress, and subjective interpretations of best interest further complicate these decisions. While DBTs represent a breakthrough in precision medicine, their role in navigating the ethical complexities of UWS is limited, emphasizing the need for integrated approaches that combine technological innovation with ethical and psychological support for proxies.
Problematic smartphone use (PSU) has been associated with withdrawal-like symptoms and altered intrinsic neural activity (INA). While previous studies suggest that PSU affects brain function, little is known about how INA is modulated by smartphone restriction. This longitudinal fMRI study investigated group- and time-dependent changes in resting-state INA following short-term smartphone deprivation. 36 participants (aged 18-29; 22 female) were categorized into PSU (n = 19) and non-PSU (n = 17) groups using the Smartphone Addiction Scale-Short Version (SAS-SV). Resting-state fMRI scans were obtained before and after a 72-hour period of smartphone restriction. Psychometric measures included the Mannheim Craving Scale (MaCS) and the Smartphone Addiction Inventory (SPAI). A significant group-by-time interaction revealed INA changes in the left inferior frontal gyrus, bilateral posterior cingulate cortex, right middle frontal and precentral gyri, and left calcarine cortex. INA increased over time in the non-PSU group but decreased in the PSU group in prefrontal and cingulate areas. In contrast, sensorimotor and occipital regions showed increased INA over time in PSU individuals. Associations between neural activity and MaCS scores indicated that greater craving was linked to reduced INA in the posterior cingulate cortex. Within the PSU group, higher smartphone-use severity, as measured by the SPAI, was associated with altered INA in occipital, parietal, and cerebellar regions. These findings suggest PSU is linked to distinct and state-dependent neurofunctional alterations that may reflect withdrawal-related processes and maladaptive reward and cognitive control mechanisms.

In recent years, many sociological, psychological, and epidemiological studies have focused on the syndrome of social inequality, status concerns, and the emergence of social problems in affluent capitalist societies. The basic assumption is that increasing competitive pressures stress people and cause them to seek any small advantage in the status competition. Against this background, this study examines the relationship between status seeking, status anxiety, and a competitive working climate and the disposition to engage in self-optimizing behavior. Using representative survey data from the working population in Germany (N = 3551), we show that an individual's disposition to seek high status is positively associated with self-optimization dispositions in the form of a greater willingness to use prescription drugs without medical necessity with the aim of enhancing cognitive performance. This effect is moderated by status anxiety and a competitive working climate—that is, anxious status seekers and status seekers in competitive jobs are particularly willing to self-optimize. These findings underscore the importance of positive status experiences (feeling valued), especially for highly ambitious individuals, at the work place.
Background:
Schizophrenia is one of the most severe and costly mental disorders in terms of human suffering and societal expenditure. About 15-30% of patients do not respond to all known antipsychotics, including clozapine, the current gold standard in these cases. Electroconvulsive therapy (ECT) is well-known to be highly effective in clozapine-treatment-resistant schizophrenia (CRS), and synergistic effects of clozapine and ECT have been demonstrated. However, relapse rates after successful courses of ECT are still very high, and evidence for maintenance ECT (mECT) in CRS is scarce at best.
Methods:
Here, we present the protocol of the MECT-RESIST trial, a German multi-center, observer-blind, randomized, and actively controlled parallel-group clinical trial. The scientific aim of the study is to test the hypothesis that mECT plus treatment as usual (TAU) (intervention group) is superior to TAU alone (control group) for relapse prevention in CRS. The primary endpoint is time to relapse. Secondary endpoints include the proportion of relapse-free patients, the global level of functioning and quality of life, depressive symptoms, overall symptoms of schizophrenia, concomitant catatonic symptoms, stress and self-stigmatization and cognitive performance. We aim at randomizing 84 patients between 18 and 65 years with a clinically diagnosed CRS and brief psychotic rating scale (BPRS) > 45, who responded to a series of ECT (BPRS < 70% of initial BPRS), to either recieve mECT + TAU or TAU over a period of 28 weeks followed by a follow-up of 12 months. The study will be performed between 2025 and 2028.
Discussion:
In this multi-center trial, we aim to examine the effectiveness of mECT in CRS patients who improved after a course of routine ECT. If mECT will lead to a longer time to relapse and/or to a higher proportion of relapse-free patients compared to those undergoing treatment as usual, this trial would have an enormous impact on therapeutic strategies for patients with CRS and would induce a profound change of current treatment guidelines, where ECT still ranks at the level of ultima ratio, despite accumulating evidence suggesting otherwise.
Trial registration:
ClincalTrials.gov NCT06456983, registered 7 Jun 2024. Deutsches Register Klinischer Studien DRKS00036886, registered 14 May 2025.

Objective
Delusional disorders (DD) are among the most debilitating mental disorders in the elderly. Persistent monothematic delusions frequently include paranoid and persecutory beliefs, as well as various forms of somatic delusions, including delusions of being infested by pathogens. So far, little is known about the neural correlates of DD. Yet, particularly in elderly patients, white‐matter lesions (WML) are thought to play an important pathophysiological role.
Methods
To investigate regional WML in patients with DD, structural MRI was used, followed by automated lesion segmentation methods to facilitate WML load (WMLL) comparisons between healthy controls (HC, n = 28) and patients with distinct types of DD, that is, somatic (n = 16) versus non‐somatic DD (n = 17). Patients with somatic DD presented with specific delusional content, that is, beliefs of delusional infestation (DI), whereas individuals with non‐somatic DD (non‐DI) showed predominantly paranoid and persecutory content.
Results
Regions with higher WMLL in both DI and non‐DI patients compared to HC included the anterior cingulate and lateral prefrontal regions located in the middle frontal gyrus. Regions with higher WMLL in DI patients versus both HC and non‐DI patients were predominantly located in the sensorimotor areas of the frontal lobe.
Conclusion
The data suggest distinct patterns of regional WMLL in elderly patients with DI versus non‐DI. The anatomical distribution of WMLL supports a neuromechanistic model that emphasises the importance of brain areas that drive the internal bodily focus of somatic delusions versus the externalised cognitive distortions that can be observed in non‐somatic delusions.
Using selected clinical scenarios in neuromedicine, this book demonstrates how scholarly reflection in the field of neuroethics can be applied in practice. It is primarily intended for physicians and all other healthcare professionals who encounter ethical issues in neuromedicine that arise specifically within their field of practice. By focusing on the clinical context, the book bridges the gap between introductory texts and scholarly handbooks on neuroethics. For this fully updated second edition, the broad range of topics has been expanded to include a chapter on the current use of artificial intelligence in neuromedicine.
Edited by a hospital neurologist and a research-based neuroethicist, the book features contributions from experts across various disciplines and countries.
Background:
Extraintestinal symptoms (EIS) in inflammatory bowel diseases, including fatigue, depression and anxiety, are highly prevalent, but poorly understood. Alterations of brain function may contribute to EIS, but their association with disease activity is unclear. This study analyzed intrinsic neural activity (INA) of individuals with Crohn's disease (CD) in different disease states and examined the relationship between INA and EIS.
Methods:
Patients with CD (n = 92) and healthy controls (n = 41) underwent functional magnetic resonance brain imaging and completed symptom-specific psychometry. Temporal (amplitude of low-frequency fluctuations, ALFF) and spatial (regional homogeneity, ReHo) markers of INA were compared between CD and controls and between active (patients with active Crohn's disease [aCD]) versus remitted (rCD) disease. Regression analyses explored disease-state-dependent associations between INA and EIS.
Results:
Patients exhibited aberrant INA in frontotemporal, occipital, and thalamic regions. Patients with aCD exhibited lower ALFF in left subcallosal cortex and inferior temporal gyri compared to rCD. Regional homogeneity in aCD was lower in left medial orbital gyrus and higher in right superior frontal, left inferior temporal, and left precentral gyrus. Compared to rCD, aCD showed higher ALFF predominantly in superior, ventro-, and dorsolateral prefrontal regions. Distinct associations between INA and EIS were detected in patients, particularly in the remitted state.
Conclusions:
Intrinsic brain function in patients with CD varies by disease state, with prominent frontal cortex changes in active disease. These brain activity changes are at least partly related to the magnitude of neuropsychiatric symptoms and highlight a role of disturbed brain-gut interactions in the development of EIS especially in rCD.
Background:
Auditory verbal hallucinations are a major burden for patients with schizophrenia spectrum disorder and are often resistant to pharmacological and psychotherapeutic interventions. Repetitive transcranial magnetic stimulation (rTMS) of the temporo-parietal cortex has been proposed as a treatment for persistent auditory verbal hallucinations. We aimed to compare the efficacy and safety of bilateral continuous theta burst stimulation (cTBS), a brief and efficient form of rTMS, in adults with auditory verbal hallucinations versus sham cTBS.
Methods:
This multicentre, randomised, sham-controlled, triple-blind phase 3 clinical trial was conducted at seven German psychiatric university hospitals and followed a planned two-stage adaptive design. Eligible patients were aged 18–65 years, had experienced persistent auditory verbal hallucinations at least once per week for a minimum of 3 months, and scored 3 points or higher on item P3 (hallucinatory behaviour) of the clinician-rated Positive Scale of the Positive and Negative Syndrome Scale (PANSS). 138 adults with treatment-persistent auditory verbal hallucinations and schizophrenia spectrum disorder were randomly assigned (1:1) to receive 15 sessions of active (n=70) or sham cTBS (n=68) administered sequentially as 600 pulses to the left and 600 pulses to the right temporo-parietal cortex over a 3-week period. The primary outcome was the change in the auditory hallucinations subscale of the Psychotic Symptom Rating Scales (PSYRATS-AH) from baseline to the end of treatment at 3 weeks, analysed in the intention-to-treat population, which included all randomly assigned patients who received at least one stimulation session. Safety was assessed in all patients who received at least one stimulation session. Follow-up assessments were performed at 1, 3, and 6 months after the end of treatment. People with lived experience were not involved in the study. This trial was registered at ClinicalTrials.gov, NCT02670291.
Findings:
Between Oct 24, 2015, and May 1, 2023, 2583 patients were screened for eligibility, of whom 138 patients were randomly assigned to active cTBS (n=70; 32 [46%] females and 38 [54%] males) or sham treatment (n=68;
24 [35%] females and 44 [65%] males). Race and ethnicity data were not collected. The primary intention-to-treat analysis (66 patients in the active cTBS group; 64 patients in the sham cTBS group), combining stages 1 and 2, showed patients in the active cTBS group had a significantly greater decrease in the PSYRATS-AH score at end of treatment than did patients in the sham cTBS group (–6·36 [SD 7·97] vs –3·74 [SD 5·79]; adjusted difference –2·36 [95% CI –4·71 to –0·01]; p=0·042). Overall, 85 adverse events (43 in the active cTBS group; 42 in the sham cTBS group) were reported in 22 (33%) of 66 patients in the active cTBS group and 21 (33%) of 64 patients in the sham cTBS group. Headache was the most common adverse event in both groups (n=13 active cTBS group vs n=17 sham cTBS group). One serious adverse event occurred in the active group.
Interpretation:
Sequential bilateral temporo-parietal cTBS over 3 weeks was safe and effective for reducing auditory verbal hallucinations in adults with schizophrenia spectrum disorder. This trial establishes cTBS as a treatment option for the care of these patients. Further research is needed to evaluate maintenance strategies, identify treatment predictors, and assess long-term efficacy.
Background
Neurological soft signs (NSS) are subtle sensorimotor abnormalities that have been observed in various mental disorders with neurodevelopmental origin. While NSS have been extensively examined in patients with schizophrenia (SZ), preliminary evidence also suggests that NSS are also present in patients with borderline personality disorder (BPD). However, a transdiagnostic examination of the severity of NSS in BPD compared to SZ is still lacking.
Methods
Here, NSS were examined with the Heidelberg NSS scale (HNSS) in three groups of female subjects: BPD (n = 45), SZ (n = 30) and healthy controls (HC) (n = 32). Multivariate analysis of variance (MANOVA) was conducted jointly for BPD, SZ, and HC and HNSS subscores. Post hoc tests were performed using linear discriminant analysis (LDA). In the BPD group, partial Spearman correlations (with age and medication as covariates) were performed between NSS scores and depressive symptoms (HAMD-21), impulsivity (BIS-11), dissociative symptoms (DTS), childhood trauma (CTQ), and borderline symptoms (BSL-23).
Results
BPD showed significantly higher NSS levels compared to HCs. For the BPD, significant associations between NSS and childhood trauma and depressive symptoms were found. MANOVA showed a significant group difference, LDA differentiated between HC, and patients with SZ and BPD, but not between the patient groups.
Conclusions
Patients with BPD have significantly higher NSS levels than HC. NSS in BPD showed significant associations with childhood trauma, supporting a “two-hit” model. Importantly, patients with BPD and SZ may show similar NSS patterns, suggesting that sensorimotor dysfunction is a transdiagnostic phenomenon.
BACKGROUND
Respecting patient autonomy and delivering goal-concordant care require an understanding of individual preferences. However, the preferences of incapacitated patients are often unknown and substituted judgment is fraught with high levels of inaccuracy. Ethicists have suggested a patient preference predictor (PPP) trained with machine learning (ML) to increase the accuracy of substituted judgment, but one has not yet been developed. Here, we present the first proof of concept of an ML-based PPP.
METHODS
Using population-representative data from 1811 Swiss participants of the Survey of Health, Ageing and Retirement in Europe, we evaluated several ML techniques to create a PPP and we employed a commonly used, explainable ML method to identify the best-performing model. Reflecting different use scenarios, we trained three models: a simple model based on demographic data; a clinical model trained on data that are likely to be available in electronic health records; and a personalized model incorporating richer information on individual preferences.
RESULTS
All three models outperformed the partners of index persons in our sample in accurately predicting whether the person would prefer cardiopulmonary resuscitation in the event of cardiorespiratory arrest. With a mean fivefold cross-validated accuracy of up to 70.6% (standard deviation ±1.3%), our models also performed on par with or better than typical estimates of surrogate predictive accuracy in the literature.
CONCLUSIONS
This study demonstrates that an ML-based PPP can improve surrogate decision-making. While highlighting technical and conceptual limitations, we hold this to be a major contribution to the efforts to improve care and fully respect patient autonomy.

Neuromodulation refers to the targeted, continuous, and controllable modulation of neural processes with the aim of producing therapeutic effects. A prime example of neuromodulation is deep brain stimulation (DBS). DBS is most commonly used for movement disorders, but is increasingly being applied to other neurological and psychiatric conditions as well. This article introduces the fundamentals of neuromodulation and the criteria for its ethical evaluation. It then explains current clinical and ethical considerations of neuromodulation using DBS as an example. The challenges of the procedure are illustrated using examples of DBS for depression and its effects on interpersonal relationships. The article concludes with recommendations for research and the clinical advancement of DBS.
With advances in neurotechnology and its use for medical treatment and beyond, it is important to understand the public’s awareness of such technologies and potential disparities in self-reported knowledge, because knowledge is known to influence the acceptance and use of new technologies. This study utilizes a large sample (N = 10,339) to depict the existence and extent of self-reported knowledge of these neurotechnologies and to examine knowledge disparities between respondents. Results show that most respondents self-reported at least some knowledge of ultrasound and electroencephalography (EEG), but limited knowledge of BCIs. Prior use, being a healthcare professional, and health literacy increased the odds of self-reporting some knowledge. Also gender and age disparities exist. These findings may help identify uninformed groups in society and enhance information campaigns.

Deep Brain Stimulation (DBS) represents a key area of neuromodulation that has gained wide adoption for the treatment of neurological and experimental testing for psychiatric disorders. It is associated with specific therapeutic effects based on the precision of an evolving mechanistic neuroscientific understanding. At the same time, there are obstacles to achieving symptom relief because of the incompleteness of such an understanding. These obstacles are at least in part based on the complexity of neuropsychiatric disorders and the incompleteness of DBS devices to represent prosthetics that modulate the breadth of pathological processes implicated in these disorders. Neuroprostheses, such as an implanted DBS system, can have vast effects on subjects in addition to the specific neuropsychiatric changes they are intended to produce. These effects largely represent blind spots in the current debate on neuromodulation. Anthropological accounts can illustrate the broad existential dimensions of patients’ illness and responses to neural implants. In combination with current neuroscientific understanding, neuropsychiatric anthropology may illuminate the possibilities and limits of neurodevices as technical “world enablers”.

Culturally diverse societies often struggle with providing appropriate dementia care. Cultural sensitivity is considered an important prerequisite for meeting the needs of persons with dementia. This article discusses culture specific aspects of dementia care by referring to the Turkish community in Germany as an example. Factors are discussed that specifically infringe on the quality of dementia care for migrants. The article defends the claim that good dementia care for migrants can be provided through a person-centered approach which is again based on culturally sensitive approach. We show how culture shapes health phenomena but also argue that a focus on culture may stereotype individuals as belonging to a particular culture, grouping people together irrespective of their heterogeneity. Person-centered care is ideal for recognizing diverse needs and values. It is often seen as being at odds with culturally sensitive care, but this paper suggests a way of reconciling them. We argue that culture does indeed provide a framework to create the necessary foundation for person-centered care. Finally, some criticisms and plausible replies are discussed and practical implications arising from the analysis are presented.

Human augmentation is defined as the use of science or technology to modify human performance temporarily, or permanently, to exceed normal physical and/or psychological capabilities of a human body. Our previous work proposed nine ethical principles of human augmentation in the defence context: necessity, human dignity, informed consent, transparency and accountability, equity, privacy, ongoing review, international law, and broader social impact. Here we describe the results of a mixed-methods study using focus groups (NGroups = 9) and a web-based survey among serving military personnel (NParticipants = 43) examining how important and appropriate the participants thought the principles were when considering the development, adoption, and implementation of human augmentation technology. This study explores the participants’ stated reasons for their ratings, and the association with indicators of experience and socio-demographic groups. This work provides insights into how the principles can relate to each other at various stages of the technology life cycle, and how they could function together to support a thorough ethical analysis during the implementation of such technology. Following our analysis, several refinements to the principles are subsequently suggested.
While trust is foundational to the doctor-patient relationship, the introduction of AI into healthcare settings poses the risk of eroding this trust, and such erosion cannot be countered simply by appealing to the notion of “trustworthy AI.” We argue that trust presupposes specific epistemic attitudes that cannot be meaningfully applied to AI systems. Accordingly, our focus is not on specifying which capabilities AI must exhibit in order to appear trustworthy, but on examining from an epistemological perspective how the use of AI reshapes the dynamics of trust within the doctor-patient relationship. To this end, we first sketch conceptions of trust and demonstrate how trust differs from reliance. We then combine the model of Computational Reliabilism with an epistemic framework to develop a matrix for the ethical analysis of our use cases. Finally, we apply this framework to three scenarios of melanoma detection, risk prediction, and psychotherapy chatbots, which we construct by mapping epistemic stances across different modes of human-machine interaction, ranging from collaborative support with varying degrees of autonomy to the replacement of human-human interaction. We argue that the application of AI in the doctor-patient relationship exposes what we call a “reliability gap” — a conceptual space where the opaque nature of advanced AI systems prevents both doctors and patients from independently verifying their reliability. This creates a dynamic where reliability in the AI’s performance is increasingly mediated by the doctor as a proxy. Our use cases demonstrate that the more autonomous and opaque AI systems are, the more trust in the doctor becomes essential for bridging reliability gaps, while threatening to overburden the doctor’s central role.
There has been speculation about a growing demand for substances used without medical need for cognitive enhancement (CE). Thus, the prevalence rates and the identification of sociodemographic groups at risk of this behavior need further description and constant monitoring. We conducted a nationwide web-based representative sample (N = 22,101) (regarding sex, age, education, and federal state) of the general adult population in Germany. Results show a high past twelve months prevalence of consuming caffeinated drinks for CE (62.4% of respondents), followed by food supplements and home remedies (31.4%), and caffeine tablets (2.5%). The twelve-month prevalence of CE with prescription drugs was 3.7% (lifetime: 5.5%), of whom 29.1% reported using them 40 or more times; 40.5% of all respondents indicated some future intake willingness. Cannabis was the most frequently reported illegal drug for CE (past twelve months: 4.0%; lifetime: 10.7%), followed by the category amphetamine and methamphetamine (past twelve months: 1.0%; lifetime: 2.4%), and cocaine (past twelve months: 0.9; lifetime: 2.4%). We also show variation in the prevalence across multiple ascribed and achieved sociodemographic characteristics. These results can inform public policy and prevention strategies regarding the continued monitoring of the prevalence of CE and the identification of groups at risk of drug misuse.

The new European Medical Device Regulation (MDR), i.e. Regulation (EU) 2017/745, came into force in May 2021 and is being gradually implemented, with full compliance required for all medical devices on the EU market by May 2028. One key objective of the MDR is to regulate devices that, while technically being similar or even identical to medical devices, do not (yet) have an explicit clinical purpose. Under the previous regulatory framework, the Medical Device Directive (MDD), Non-Invasive Brain Stimulation (NIBS) devices with a medical purpose were classified as medical devices and subjected to regulatory control. However, when the same NIBS devices were used for non-medical purposes, such as cognitive enhancement in healthy individuals or experimental research on healthy participants, they were not regulated, despite posing the same risks. The new MDR aims to address this gap by extending regulatory control to such "non-medical devices", enhancing user safety through "more stringent” conformity assessment and post-market surveillance and ensuring that unsafe or non-compliant devices do not reach the public market.
Annex XVI of the MDR lists devices that fall under the scope of the law, even though they are lacking an intended medical purpose. The list includes: “Equipment intended for brain stimulation that apply electrical currents or magnetic or electromagnetic fields that penetrate the cranium to modify neural activity in the brain.“ This category encompasses all forms of transcranial electrical stimulation (tES), including direct current, alternating current and random noise stimulation (tDCS, tACS, and tRNS) and transcranial magnetic stimulation (TMS). Notably, neither the list in Annex XVI nor their reclassification include more recently introduced technologies that employ other physical principles to non-invasively stimulate the human brain, such as transcranial ultrasonic stimulation (TUS) or photobiomodulation (PBM). While Annex XVI had listed the transcranial electrical and magnetic stimulation technologies in 2017, the risk classification for these devices, when being used for non-medical purposes, remained unspecified for several years. This left industry and researchers in limbo as they awaited final decisions from the EU.
Under the MDR, medical devices are classified into four classes following a risk-based classification scheme, which links the class of the device to the potential risk posed to the patient's health due to performance faults. All medical devices are classified as class I, IIa, IIb, or III, with class III being the highest risk class. Class III devices are per definition those where a malfunction or failure of the device could result in death or serious injury. These are primarily devices intended for invasive surgical procedures, such as deep brain stimulators or pacemakers. Guidance documents, published in 2021, clarified that NIBS technologies used for clinical or medical purposes (and thus covered by the core of the MDR rather than Annex XVI), were classified as Class IIa (i.e., TMS and low intensity tES) or Class IIb (see MDCG 2021-24).3 It was therefore widely assumed that the classification of these types of NIBS devices would have the same or lower classification for non-medical use, as patients are generally considered to be at higher risk due to their overall health status, but this assumption proved incorrect, even the reverse came up.
While we agree that the risk-benefit ratio of NIBS devices may be higher and harder to control when used unsupervised by non-experts, the reclassification was based on the premise of “increased risk”. This has led to widespread confusion in the brain stimulation field, slowing research, leaving clinicians uncertain, and frustrating patients [1,2].
The aim of this paper is i) to review the scientific evidence on the basis of which reclassification was implemented and provide the relevant scientific proof that was omitted; ii) to summarize our efforts how we have tried to act against the reclassification; iii) to present clear, evidence-based findings to address existing ambiguities in the regulatory NIBS field, providing the scientific community with reliable information to guide further research and application. This is relevant as any risk assessment and claims of possible side and adverse effects should be based on scientific empirical data rather than speculation. The “saga” until now was mainly about procedures and regulatory processes and thus, on formalities. What is missing is a scientific review of the concrete articles and evidence put forward by the reclassification committee to justify their revised risk assessment of NIBS. The current article is written by leading experts, scientists who evaluated this evidence and provide a pure scientific assessment of the data we have available today.

While risk perceptions affect various health behaviors, there is insufficient knowledge about how they are formed and change over time surrounding illicit substance use. This study investigates the role of prior use, social influences, and media information on changes in the risk perceptions of expected susceptibility and severity of side effects in the context of the nonmedical use of prescription drugs for cognitive enhancement. It also examines differential updating by testing for the potential conditioning effects of prior use and self-control. We use a three-wave panel design (N = 8,377) with a nationwide random sample of adults in Germany. Fixed-effect regression models show that prior use and positive media information lower both risk perceptions, while negative information from others and the media produce increases. Rare users compared to non- and frequent users were more sensitive to new information obtained through others, thus showing stronger changes in risk perceptions. Moreover, self-control partially moderated the magnitude of changes in both risk perceptions, for example, regarding side effects reported in the media, which affected individuals with low self-control more strongly. In sum, the results indicate that personal and vicarious information affect the updating of risk perceptions, while partial evidence exists for differential updating.

Background
The use of artificial intelligence (AI) in psychiatry holds promise for diagnosis, therapy, and the categorization of mental disorders. At the same time, it raises significant theoretical and ethical concerns. The debate appears polarized, with proponents and critics seemingly irreconcilably opposed. On the one hand, AI is heralded as a transformative force poised to revolutionize psychiatric research and practice. On the other hand, it is depicted as a harbinger of dehumanization. To better understand this dichotomy, it is essential to identify and critically examine the underlying arguments. To what extent does the use of AI challenge the theoretical assumptions of psychiatric diagnostics? What implications does it have for patient care, and how does it influence the professional self-concept of psychiatrists?
Methods
To explore these questions, we conducted 15 semi-structured interviews with experts from psychiatry, computer science, and philosophy. The findings were analyzed using a structuring qualitative content analysis.
Results
The analysis focuses on the significance of AI for psychiatric diagnosis and care, as well as on its implications for the identity of psychiatry. We identified different lines of argument suggesting that expert views on AI in psychiatry hinge on the types of data considered relevant and on whether core human capacities in diagnosis and treatment are viewed as replicable by AI.
Conclusions
The results provide a mapping of diverse perspectives, offering a basis for more detailed analysis of theoretical and ethical issues of AI in psychiatry, as well as for the adaptation of psychiatric education.
Purpose
This study aims to demonstrate the importance of recognizing stress in the workplace. Accurate novel objective methods that use electroencephalogram (EEG) to measure brainwaves can promote employee well-being. However, using these devices can be positive and potentially harmful as manipulative practices undermine autonomy.
Design/methodology/approach
Emphasis is placed on business ethics as it relates to the ethics of action in terms of positive and negative responsibility, autonomous decision-making and self-determined work through a literature review. The concept of relational autonomy provides an orientation toward heteronomous employment relationships.
Findings
First, using digital devices to recognize stress and promote health can be a positive outcome, expanding the definition of digital well-being as opposed to dependency, non-use or reduction. Second, the transfer of socio-relational autonomy, according to Oshana, enables criteria for self-determined work in heteronomous employment relationships. Finally, the deployment and use of such EEG-based devices for stress detection can lead to coercion and manipulation, not only in interpersonal relationships, but also directly and more subtly through the technology itself, interfering with self-determined work.
Originality/value
Stress at work and EEG-based devices measuring stress have been discussed in numerous articles. This paper is one of the first to explore ethical considerations using these brain–computer interfaces from an employee perspective.
This book offers a comprehensive review of current topics in decision making. It covers new findings relating to foundations, mechanisms, and consequences of decisions, shedding light on the cognitive processes from different disciplinary perspectives. Chapters report on psychological studies of the cognitive mechanisms of decision making, neuroimaging studies on the neural correlates, studies of patient populations to characterize alterations in decision making in specific diseases, as well as discussions concerning philosophical and ethical issues.
In recent debates on digital twins, much attention has been paid to understanding the interaction between individuals and their digital representations (Braun, Citation2021). Iglesias et al. (Citation2025) shed new light on this debate, extending the reflection on digital doppelgängers—digital twins that try to replicate the psychological dimension of an individual. They argue that such copies may serve as valuable means to achieve legacy and relational aims left unaddressed due to the person’s death. Against this background, we discuss how far we may better understand the implied normative aspects by considering them in terms of the represented person’s death. Specifically, we ask how we can and should, in normative terms, deal with a digital twin as a representation of a person after their death.
Here, we consider the decommissioning of such technology. We define decommissioning as the withdrawal, dismantling, or rendering the doppelgänger incapable of serving its original aims. We hypothesize that the way in which these digital doppelgängers ought to be decommissioned may depend upon whether they are viewed either as a proxy or as an extension of personhood. By proxy, we mean a stand-in for an individual by replicating their decisions and style without embodying their personal identity or subjective experience; something that makes decisions on your behalf but is not you (Braun and Krutzinna Citation2022). What is left behind is akin to an artifact owned by you. Whereas an extension of personhood can mean extending aspects of an individual’s identity and relational presence beyond death by reflecting their values, projects, and relationships; something that is/was a part of yourself. What is left behind is akin to an “informational corpse” (Öhman and Floridi Citation2018).
Answering this decommissioning question is necessary not only to respect the intended aims of those for whom the digital doppelgängers were created, but also to potentially respect certain social norms surrounding obsequies. Viewing digital doppelgängers either as proxies or extensions of personhood implies respective normative notions. For instance, the pursuit of any decommissioning strategy will require necessary and sufficient standards of informed consent, which may be difficult to parse given that not all individuals will view their digital doppelgänger in the same manner. The decommissioning of digital doppelgängers is thus enriched by moral nuances influenced by the perceptions we may have of this technology.
Optogenetics has potentials for a treatment of retinitis pigmentosa and other rare degenerative retinal diseases. The technology allows controlling cell activity through combining genetic engineering and optical stimulation with light. First clinical studies are already being conducted, whereby the vision of participating patients who were blinded by retinitis pigmentosa was partially recovered. In view of the ongoing translational process, this paper examines regulatory aspects of preclinical and clinical research as well as a therapeutic application of optogenetics in ophthalmology. There is no prohibition or specific regulation of optogenetic methods in the European Union. Regarding preclinical research, legal issues related to animal research and stem cell research have importance. In clinical research and therapeutic applications, aspects of subjects' and patients' autonomy are relevant. Because at EU level, so far, no specific regulation exists for clinical studies in which a medicinal product and a medical device are evaluated simultaneously (combined studies) the requirements for clinical trials with medicinal products as well as those for clinical investigations on medical devices apply. This raises unresolved legal issues and is the case for optogenetic clinical studies, when for the gene transfer a viral vector classified as gene therapy medicinal product (GTMP) and for the light stimulation a device qualified as medical device are tested simultaneously. Medicinal products for optogenetic therapies of retinitis pigmentosa fulfill requirements for designation as orphan medicinal product, which goes along with regulatory and financial incentives. However, equivalent regulation does not exist for medical devices for rare diseases.

Virtual reality (VR) induces a radical psychological reorientation. Yet descriptions of this reorientation are often steeped in theoretically misleading metaphors. We offer a more measured account, grounded in both philosophy and cognitive psychology, and use it to access the claim that VR promotes moral learning by simulating another's perspective. This hypothesis depends on the assumption that avatar use produces experiences sufficiently similar to those of others to enable empathic growth. We reject that assumption and offer two arguments against it. Empathy relevant to moral learning requires interpretive effort and contextual understanding, not just a shift in perspective. And VR's open-ended, user-driven structure tends to reinforce prior assumptions rather than unsettle them. Still, avatar use may have a different effect on moral learning, which we call self-fragmentation. By loosening the boundaries of the self, VR may expand the range of people one is disposed to empathize with.
When making substituted judgments for incapacitated patients, surrogates often struggle to guess what the patient would want if they had capacity. Surrogates may also agonize over having the (sole) responsibility of making such a determination. To address such concerns, a Patient Preference Predictor (PPP) has been proposed that would use an algorithm to infer the treatment preferences of individual patients from population-level data about the known preferences of people with similar demographic characteristics. However, critics have suggested that even if such a PPP were more accurate, on average, than human surrogates in identifying patient preferences, the proposed algorithm would nevertheless fail to respect the patient's (former) autonomy since it draws on the 'wrong' kind of data: namely, data that are not specific to the individual patient and which therefore may not reflect their actual values, or their reasons for having the preferences they do. Taking such criticisms on board, we here propose a new approach: the Personalized Patient Preference Predictor (P4). The P4 is based on recent advances in machine learning, which allow technologies including large language models to be more cheaply and efficiently 'fine-tuned' on person-specific data. The P4, unlike the PPP, would be able to infer an individual patient's preferences from material (e.g., prior treatment decisions) that is in fact specific to them. Thus, we argue, in addition to being potentially more accurate at the individual level than the previously proposed PPP, the predictions of a P4 would also more directly reflect each patient's own reasons and values. In this article, we review recent discoveries in artificial intelligence research that suggest a P4 is technically feasible, and argue that, if it is developed and appropriately deployed, it should assuage some of the main autonomy-based concerns of critics of the original PPP. We then consider various objections to our proposal and offer some tentative replies.

Background
Artificial intelligence (AI) has revolutionized various healthcare domains, where AI algorithms sometimes even outperform human specialists. However, the field of clinical ethics has remained largely untouched by AI advances. This study explores the attitudes of anesthesiologists and internists towards the use of AI-driven preference prediction tools to support ethical decision-making for incapacitated patients.
Methods
A questionnaire was developed and pretested among medical students. The questionnaire was distributed to 200 German anesthesiologists and 200 German internists, thereby focusing on physicians who often encounter patients lacking decision-making capacity. The questionnaire covered attitudes toward AI-driven preference prediction, availability and utilization of Clinical Ethics Support Services (CESS), and experiences with ethically challenging situations. Descriptive statistics and bivariate analysis was performed. Qualitative responses were analyzed using content analysis in a mixed inductive-deductive approach.
Results
Participants were predominantly male (69.3%), with ages ranging from 27 to 77. Most worked in nonacademic hospitals (82%). Physicians generally showed hesitance toward AI-driven preference prediction, citing concerns about the loss of individuality and humanity, lack of explicability in AI results, and doubts about AI’s ability to encompass the ethical deliberation process. In contrast, physicians had a more positive opinion of CESS. Availability of CESS varied, with 81.8% of participants reporting access. Among those without access, 91.8% expressed a desire for CESS.
Physicians' reluctance toward AI-driven preference prediction aligns with concerns about transparency, individuality, and human-machine interaction. While AI could enhance the accuracy of predictions and reduce surrogate burden, concerns about potential biases, de-humanisation, and lack of explicability persist.
Conclusions
German physicians frequently encountering incapacitated patients exhibit hesitance toward AI-driven preference prediction but hold a higher esteem for CESS. Addressing concerns about individuality, explicability, and human-machine roles may facilitate the acceptance of AI in clinical ethics. Further research into patient and surrogate perspectives is needed to ensure AI aligns with patient preferences and values in complex medical decisions.
A significant amount of European basic and clinical neuroscience research includes the use of transcranial magnetic stimulation (TMS) and low intensity transcranial electrical stimulation (tES), mainly transcranial direct current stimulation (tDCS). Two recent changes in the EU regulations, the introduction of the Medical Device Regulation (MDR) (2017/745) and the Annex XVI have caused significant problems and confusions in the brain stimulation field. The negative consequences of the MDR for non-invasive brain stimulation (NIBS) have been largely overlooked and until today, have not been consequently addressed by National Competent Authorities, local ethical committees, politicians and by the scientific communities. In addition, a rushed bureaucratic decision led to seemingly wrong classification of NIBS products without an intended medical purpose into the same risk group III as invasive stimulators.
Overregulation is detrimental for any research and for future developments, therefore researchers, clinicians, industry, patient representatives and an ethicist were invited to contribute to this document with the aim of starting a constructive dialogue and enacting positive changes in the regulatory environment.
This volume focuses on the ethical dimensions of the technological framework in which human thought and action is embedded and which has been brought into the focus of cognitive science by theories of situated cognition. There is a broad spectrum of technologies that co-actualize or enable and reinforce human cognition and action and that differ in the degree of physical integration, interactivity, adaptation processes, dependency and indispensability, etc. This technological framework of human cognition and action is evolving rapidly. Some changes are continuous, others are eruptive. Technologies that use machine learning, for example, could represent a qualitative leap in the technological framework of human cognition and action. The ethical consequences of applying theories of situated cognition to practical cases have not yet received adequate attention and are explored in this volume.
Non-invasive brain stimulation (NIBS) techniques such as transcranial direct current stimulation (tDCS) or transcranial magnetic stimulation (TMS) have made great progress in recent years and offer boundless potential for the neuroscientific research and treatment of disorders. However, the possible use of NIBS devices for neuro-doping and neuroenhancement in healthy individuals and the military are poorly regulated. The great potentials and diverse applications can have an impact on the future development of the technology and society. This participatory study therefore aims to summarize the perspectives of different stakeholder groups with the help of qualitative workshops. Nine qualitative on-site and virtual workshops were conducted in the study with 91 individuals from seven stakeholder groups: patients, students, do-it-yourself home users of tDCS, clinical practitioners, industry representatives, philosophers, and policy experts. The co-creative and design-based workshops were tailored to each group to document the wishes, fears, and general comments of the participants. The outlooks from each group were collected in written form and summarized into different categories. The result is a comprehensive overview of the different aspects that need to be considered in the field of NIBS. For example, several groups expressed the wish for home-based tDCS under medical supervision as a potential therapeutic intervention and discussed the associated technical specifications. Other topics that were addressed were performance enhancement for certain professional groups, training requirements for practitioners, and questions of agency, among others. This qualitative participatory research highlights the potential of tDCS and repetitive TMS as alternative therapies to medication, with fewer adverse effects and home-based use for tDCS. The ethical and societal impact of the abuse of NIBS for non-clinical use must be considered for policy-making and regulation implementations. This study adds to the neuroethical debate on the responsible use and application of NIBS technologies, taking into consideration the different perspectives of important stakeholders in the field.
Machine learning (ML) has significantly enhanced the abilities of robots, enabling them to perform a wide range of tasks in human environments and adapt to our uncertain real world. Recent works in various ML domains have highlighted the importance of accounting for fairness to ensure that these algorithms do not reproduce human biases and consequently lead to discriminatory outcomes. With robot learning systems increasingly performing more and more tasks in our everyday lives, it is crucial to understand the influence of such biases to prevent unintended behavior toward certain groups of people. In this work, we present the first survey on fairness in robot learning from an interdisciplinary perspective spanning technical, ethical, and legal challenges. We propose a taxonomy for sources of bias and the resulting types of discrimination due to them. Using examples from different robot learning domains, we examine scenarios of unfair outcomes and strategies to mitigate them. We present early advances in the field by covering different fairness definitions, ethical and legal considerations, and methods for fair robot learning. With this work, we aim to pave the road for groundbreaking developments in fair robot learning.
Numerous complex and multi-faceted ethical questions arise from the innovation of neurotechnologies. Addressing these issues effectively requires the involvement of a diverse range of stakeholders, including patients, treatment providers, home users, scientists and engineers from different disciplines, and industry representatives. Different groups, however, possess varying levels of knowledge and experience regarding the ethical use and innovation of neurotechnologies. Therefore, customized methods are needed to identify their perspectives and ethical concerns. This article aims to introduce practical methods for eliciting ethical questions in the field of neurotechnology, including user journeys, persona approaches, material thinking, scenario building, fictional media contributions, and categorization.
With regard to the dual-use problem, digitalisation in the life sciences has two distinct influences, namely an exacerbating and an expanding one. By enabling faster and more extensive research and development processes, digitalisation exacerbates the existing dual-use problem because it also increases the speed at which the results of this research can be used for security-relevant purposes. In addition, the digitalisation of the life sciences extends the dual-use problem, as some of the digital tools that are developed and used in the life sciences can themselves be used for military or security-related purposes.
Broad-based governance is therefore required, including broad stakeholder participation in the research process and the provision of information on dual use in education in good scientific practice across institutions, career stages and disciplines.

In this letter to the editor, Antal and Baeken respond to a commentary by Rethwilm et al. on their position paper regarding the impact of the new EU Medical Device Regulation (MDR) on non-invasive brain stimulation (NIBS) research. While the authors welcome the commentators’ general agreement, they highlight ongoing challenges due to inconsistent interpretations of the MDR across countries and ethics committees. A major issue is that local ethics boards often lack legal or technical expertise, leading to bureaucratic and overly cautious decisions. Antal and Baeken call for clearer, binding guidelines and standardized procedures to harmonize research practices and reduce unnecessary barriers. The letter emphasizes the urgent need to clarify regulatory ambiguities to safeguard the future of NIBS research in Europe.
Phenomenological interview methods (PIMs) have become important tools for investigating subjective, first-person accounts of the novel experiences of people using neurotechnologies. Through the deep exploration of personal experience, PIMs help reveal both the structures shared between and notable differences across experiences. However, phenomenological methods vary on what aspects of experience they aim to capture and what they may overlook. Much discussion of phenomenological methods has remained within the philosophical and broader bioethical literature. Here, we begin with a conceptual primer and preliminary guide for using phenomenological methods to investigate the experiences of neural device users.
To improve and expand the methodology of phenomenological interviewing, especially in the context of the experience of neural device users, we first briefly survey three different PIMs, to demonstrate their features and shortcomings. Then we argue for a critical phenomenology—rejecting the ‘neutral’ phenomenological subject—that encompasses temporal and ecological aspects of the subjects involved, including interviewee and interviewer (e.g. age, gender, social situation, bodily constitution, language skills, potential cognitive disease-related impairments, traumatic memories) as well as their relationality to ensure embedded and situated interviewing. In our view, PIMs need to be based on a conception of experience that includes and emphasizes the relational and situated, as well as the anthropological, political and normative dimensions of embodied cognition.
We draw from critical phenomenology and trauma-informed qualitative work to argue for an ethically sensitive interviewing process from an applied phenomenological perspective. Drawing on these approaches to refine PIMs, researchers will be able to proceed more sensitively in exploring the interviewee’s relationship with their neuroprosthetic and will consider the relationship between interviewer and interviewee on both interpersonal and social levels.
As part of the ERANET NEURON initiative, this study conducted participatory workshops with seven stakeholder groups—including patients, clinicians, companies, home users, policy experts, and philosophers—to capture their perspectives, wishes, and concerns regarding non-invasive brain stimulation (NIBS). The qualitative findings were evaluated by an interdisciplinary expert panel and translated into recommendations for policymakers, health authorities, researchers, and industry.
The study reveals that access to NIBS in Europe is limited by unequal reimbursement policies and regulatory barriers, particularly the classification of NIBS devices as high-risk (Class III). The authors advocate for broader approval of tDCS for home use, clear standards for neurodata privacy, and EU-wide harmonization of certification and research funding. Emphasis is placed on the importance of involving all relevant stakeholders in decision-making processes to address ethical, legal, and practical challenges responsibly. The results highlight the potential of NIBS for medicine and society while underscoring the urgent need for structural adaptations.

This paper explores the potential of community-led participatory research for value orientation in the development of medical AI systems. First, conceptual aspects of participation and sharing, the current paradigms of AI development in medicine and the new challenges of AI technologies are examined. The paper proposes a shift towards a more participatory and community-led approach to AI development, illustrated by various participatory research methods in the social sciences and design thinking. It discusses the prevailing paradigms of ethics by design and embedded ethics in value customization of medical technologies and acknowledges their limitations and criticisms. It then presents a model for community-led development of AI in medicine that emphasizes the importance of involving communities at all stages of the research process. The paper argues for a shift towards a more participatory and community-led approach to AI development in medicine, which promises more effective and ethical medical AI systems.
Recent work on ecological accounts of moral responsibility and agency have argued for the importance of social environments for moral reasons responsiveness. Moral audiences can scaffold individual agents’ sensitivity to moral reasons and their motivation to act on them, but they can also undermine it. In this paper, we look at two case studies of ‘scaffolding bad’, where moral agency is undermined by social environments: street gangs and online incel communities. In discussing these case studies, we draw both on recent situated cognition literature and on scaffolded responsibility theory. We show that the way individuals are embedded into a specific social environment changes the moral considerations they are sensitive to in systematic ways because of the way these environments scaffold affective and cognitive processes, specifically those that concern the perception and treatment of ingroups and outgroups. We argue that gangs undermine reasons responsiveness to a greater extent than incel communities because gang members are more thoroughly immersed in the gang environment.
The concept of autonomy is indispensable in the history of Western thought. At least that’s how it seems to us nowadays. However, the notion has not always had the outstanding significance that we ascribe to it today and its exact meaning has also changed considerably over time. In this paper, we want to shed light on different understandings of autonomy and clearly distinguish them from each other. Our main aim is to contribute to conceptual clarity in (interdisciplinary) discourses and to point out possible pitfalls of conceptual pluralism.
Trustworthy medical AI requires transparency about the development and testing of underlying algorithms to identify biases and communicate potential risks of harm. Abundant guidance exists on how to achieve transparency for medical AI products, but it is unclear whether publicly available information adequately informs about their risks. To assess this, we retrieved public documentation on the 14 available CE-certified AI-based radiology products of the II b risk category in the EU from vendor websites, scientific publications, and the European EUDAMED database. Using a self-designed survey, we reported on their development, validation, ethical considerations, and deployment caveats, according to trustworthy AI guidelines. We scored each question with either 0, 0.5, or 1, to rate if the required information was “unavailable”, “partially available,” or “fully available.” The transparency of each product was calculated relative to all 55 questions. Transparency scores ranged from 6.4% to 60.9%, with a median of 29.1%. Major transparency gaps included missing documentation on training data, ethical considerations, and limitations for deployment. Ethical aspects like consent, safety monitoring, and GDPR-compliance were rarely documented. Furthermore, deployment caveats for different demographics and medical settings were scarce. In conclusion, public documentation of authorized medical AI products in Europe lacks sufficient public transparency to inform about safety and risks. We call on lawmakers and regulators to establish legally mandated requirements for public and substantive transparency to fulfill the promise of trustworthy AI for health.
The debate regarding prediction and explainability in artificial intelligence (AI) centers around the trade-off between achieving high-performance accurate models and the ability to understand and interpret the decisionmaking process of those models. In recent years, this debate has gained significant attention due to the increasing adoption of AI systems in various domains, including healthcare, finance, and criminal justice. While prediction and explainability are desirable goals in principle, the recent spread of high accuracy yet opaque machine learning (ML) algorithms has highlighted the trade-off between the two, marking this debate as an inter-disciplinary, inter-professional arena for negotiating expertise. There is no longer an agreement about what should be the “default” balance of prediction and explainability, with various positions reflecting claims for professional jurisdiction. Overall, there appears to be a growing schism between the regulatory and ethics-based call for explainability as a condition for trustworthy AI, and how it is being designed, assimilated, and negotiated. The impetus for writing this commentary comes from recent suggestions that explainability is overrated, including the argument that explainability is not guaranteed in human healthcare experts either. To shed light on this debate, its premises, and its recent twists, we provide an overview of key arguments representing different frames, focusing on AI in healthcare.
Position papers on artificial intelligence (AI) ethics are often framed as attempts to work out technical and regulatory strategies for attaining what is commonly called trustworthy AI. In such papers, the technical and regulatory strategies are frequently analyzed in detail, but the concept of trustworthy AI is not. As a result, it remains unclear. This paper lays out a variety of possible interpretations of the concept and concludes that none of them is appropriate. The central problem is that, by framing the ethics of AI in terms of trustworthiness, we reinforce unjustified anthropocentric assumptions that stand in the way of clear analysis. Furthermore, even if we insist on a purely epistemic interpretation of the concept, according to which trustworthiness just means measurable reliability, it turns out that the analysis will, nevertheless, suffer from a subtle form of anthropocentrism. The paper goes on to develop the concept of strange error, which serves both to sharpen the initial diagnosis of the inadequacy of trustworthy AI and to articulate the novel epistemological situation created by the use of AI. The paper concludes with a discussion of how strange error puts pressure on standard practices of assessing moral culpability, particularly in the context of medicine.
This study examines the impact of sample size on predicting cognitive and mental health phenotypes from brain imaging via machine learning. Our analysis shows a 3- to 9-fold improvement in prediction performance when sample size increases from 1,000 to 1 M participants. However, despite this increase, the data suggest that prediction accuracy remains worryingly low and far from fully exploiting the predictive potential of brain imaging data. Additionally, we find that integrating multiple imaging modalities boosts prediction accuracy, often equivalent to doubling the sample size. Interestingly, the most informative imaging modality often varied with increasing sample size, emphasizing the need to consider multiple modalities. Despite significant performance reserves for phenotype prediction, achieving substantial improvements may necessitate prohibitively large sample sizes, thus casting doubt on the practical or clinical utility of machine learning in some areas of neuroimaging.
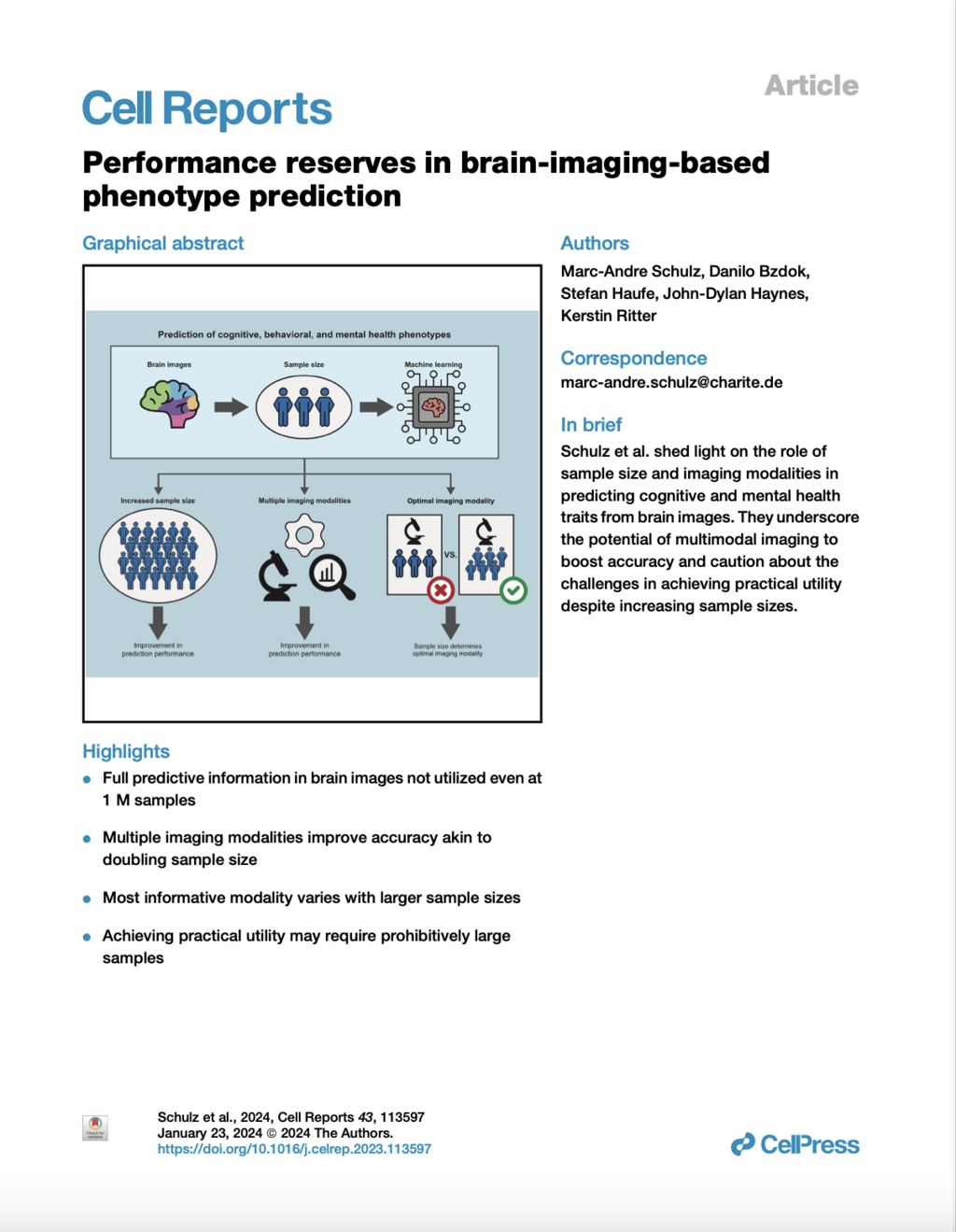

Deep Learning (DL) has emerged as a powerful tool in neuroimaging research. DL models predicting brain pathologies, psychological behaviors, and cognitive traits from neuroimaging data have the potential to discover the neurobiological basis of these phenotypes. However, these models can be biased by spurious imaging artifacts or by the information about age and sex encoded in the neuroimaging data. In this study, we introduce a lightweight and easy-to-use framework called ‘DeepRepViz’ designed to detect such potential confounders in DL model predictions and enhance the transparency of predictive DL models. DeepRepViz comprises two components - an online visualization tool (available at https://deep-rep-viz.vercel.app/) and a metric called the ‘Con-score’. The tool enables researchers to visualize the final latent representation of their DL model and qualitatively inspect it for biases. The Con-score, or the ‘concept encoding’ score, quantifies the extent to which potential confounders like sex or age are encoded in the final latent representation and influences the model predictions. We illustrate the rationale of the Con-score formulation using a simulation experiment. Next, we demonstrate the utility of the DeepRepViz framework by applying it to three typical neuroimaging-based prediction tasks (n = 12000). These include (a) distinguishing chronic alcohol users from controls, (b) classifying sex, and (c) predicting the speed of completing a cognitive task known as ‘trail making’. In the DL model predicting chronic alcohol users, DeepRepViz uncovers a strong influence of sex on the predictions (Con-score = 0.35). In the model predicting cognitive task performance, DeepRepViz reveals that age plays a major role (Con-score = 0.3). Thus, the DeepRepViz framework enables neuroimaging researchers to systematically examine their model and identify potential biases, thereby improving the transparency of predictive DL models in neuroimaging studies.
Various forms of brain stimulation are used to treat different neurological and psychiatric diseases, as well as for research purposes. In legal discourse, the focus has so far been predominantly on deep brain stimulation. In contrast, there is a lack of discussion on methods of non-invasive brain stimulation. Against the backdrop of the legal framework changed by Regulation (EU) 2017/745, this article first provides a classification under medical device law. It then explains issues of information and consent. Additionally, it presents the legal aspects of using AI in the context of non-invasive and deep brain stimulation. Finally, it provides an outlook on the methods of neural optogenetics that are still under development.

The question of whether Deep Brain Stimulation (DBS), as open-loop, closed-loop or adaptive technology, induces unwanted effects on patients’ personality is still an ongoing multidisciplinary debate. Zuk et al. (2023) findings are a reflection of this active discussion in neuroethics focussing on the specific nature of changes potentially induced by DBS/aDBS, particularly emphasizing unwanted or undesirable effects experienced by the patients based on researchers’ accounts. In their article, Zuk et al provide further evidence about the complexity of studying these DBS postoperative putative effects on personality (Pugh 2020; Zuk and Lázaro-Muñoz 2021; Gilbert, Viña, and Ineichen 2021a, 2021b). Putting aside that patients may experience unintended effects of the technology, the main debate revolves around 1) whether the known reported DBS/aDBS effects originate from the technology; and 2) whether we are looking at the right measure and outcomes.
In the study conducted by Zuk et al., it was highlighted that there exists a substantial hurdle when it comes to conceptualizing the notion of “personality.” This was evidenced by the fact that a majority of the researchers surveyed (n = 13, 57%) expressed reservations and apprehensions regarding how to define personality. The elusive nature of “personality” is apparent as it lacks definitional isomorphism across academic disciplines (Gilbert, Viña, and Ineichen 2021b). Importantly, Zuk et al. also found that most of surveyed researchers (n = 21, 91%) acknowledged the presence of changes in personality, mood, or behavior in patients who underwent DBS. This suggests that while a satisfactory definition of personality may be elusive, the observation of potential changes appears feasible, regardless of whether these changes were experienced as positive or negative by patients.
Let us consider these study outcomes for a moment: The findings of Zuk et al. shed light on the intricacies involved in attempting to quantify and measure a set of variables that lack a precise definition, and which ultimately constitute the elusive concept of personality. Despite this challenge, the observations made by clinicians and patients reveal the presence of certain variations of change related to this complex framework. In other words, a quantifiable assessment of variation is reported here despite the absence of a precise definition of the underlying concept or variables to measure. This indicates that there are ineluctable uncertainties or ambiguities in the understanding and therefore measurement of the variables at stake. This insight shows important parallels to a known debate dealing with eliminativism (or eliminative materialism) suggesting that we are attempting to measure the elusive quality of a je ne sais quoi. This je ne sais quoi involves grappling with insubstantial characteristics that are hard to capture using currently available and objective measurement tools.
Whilst eliminative theory change posits that a given notion is empty, as it refers to nothing real, conservative theory change occurs when a given notion needs a given degree of revision so that the previous notion can be abandoned in favor of a more accurate account. For this short comment it must be sufficient to state that both accounts can be, in one form or the other, associated with eliminative materialism despite blurring between eliminativism and reductionism (we refrain from outlining discussions about the various notions). The difficulty or impossibility of adequately measuring changes in personality may indicate that the concept of personality itself is misguided or potentially flawed when applied to the phenomenology of DBS.
How does knowing another team member is cognitively impaired or enhanced affect people's motivation to contribute to the team's performance? Building on the Effects of Grouping on Impairments and Enhancements (GIE) framework, we conducted two between-subjects experiments (Ntotal = 2,352) with participants from a representative, nationwide sample of the working population in Germany. We found that another group member's impairment (sleep deprivation) and enhancement (taking enhancement drugs) lowered participants’ intentions to contribute to the team's performance. These effects were mediated by lowered perceived competence (enhancement and impairment) and warmth (only enhancement) of the other group member. The reason for being impaired or enhanced (altruistic vs. egoistic reason) moderated the indirect effect of the impairment on intended effort via warmth. Our results illustrate that people's work motivation is influenced by the psychophysiological states of other group members. Hence, the enhancement of one group member can have the paradoxical effect of impairing the performance of another.
In December 2022, the European Union (EU) unexpectedly reclassified repetitive transcranial magnetic stimulation (rTMS) and transcranial electrical stimulation (tES) as Class III medical devices—the highest risk category, typically reserved for invasive procedures such as deep brain stimulation. This decision is based on a flawed risk assessment that contradicts scientific evidence: Current studies and meta-analyses confirm that rTMS and tES are safe when used correctly, with only mild and rare adverse effects. The EU’s justification includes factually incorrect claims, such as NIBS causing “atypical brain development” or “abnormal brain activity,” which are unsupported by data.
The reclassification process lacked adequate consultation with experts or NIBS manufacturers and was finalized after an eight-week public hearing that received only 22 comments—most unrelated to NIBS. This decision has severe consequences: Research projects face delays, development costs rise, and European patients risk losing access to established non-pharmacological therapies. The European Society for Brain Stimulation (ESBS) warns that this move threatens Europe’s leading role in NIBS research and demands a reversal to Class IIa (moderate risk), which aligns with the actual safety profile of NIBS. A protest letter has already been submitted to the EU; further details and support are available on the ESBS website.

As brain-computer interfaces are promoted as assistive devices, some researchers worry that this promise to “restore” individuals worsens stigma toward disabled people and fosters unrealistic expectations. In three web-based survey experiments with vignettes, we tested how refusing a brain-computer interface in the context of disability affects cognitive (blame), emotional (anger), and behavioral (coercion) stigmatizing attitudes (Experiment 1, N = 222) and whether the effect of a refusal is affected by the level of brain-computer interface functioning (Experiment 2, N = 620) or the risk of malfunctioning (Experiment 3, N = 620). We found that refusing a brain-computer interface increased blame and anger, while brain-computer interface functioning did change the effect of a refusal. Higher risks of device malfunctioning partially reduced stigmatizing attitudes and moderated the effect of refusal. This suggests that information about disabled people who refuse a technology can increase stigma toward them. This finding has serious implications for brain-computer interface regulation, media coverage, and the prevention of ableism.
The articles in this volume examine the extent to which current developments in the field of artificial intelligence (AI) are leading to new types of interaction processes and changing the relationship between humans and machines. First, new developments in AI-based technologies in various areas of application and development are presented. Subsequently, renowned experts discuss novel human-machine interactions from different disciplinary perspectives and question their social, ethical and epistemological implications. The volume sees itself as an interdisciplinary contribution to the sociopolitically pressing question of how current technological changes are altering human-machine relationships and what consequences this has for thinking about humans and technology.
Based on assumptions of the Job Demands-Resources model, we investigated employees’ willingness to use prescription drugs such as methylphenidate and modafinil for nonmedical purposes to enhance their cognitive functioning as a response to strain (i.e., perceived stress) that is induced by job demands (e.g., overtime, emotional demands, shift work, leadership responsibility). We also examined the direct and moderating effects of resources (e.g., emotional stability, social and instrumental social support) in this process. We utilized data from a representative survey of employees in Germany (N = 6454) encompassing various job demands and resources, levels of perceived stress, and willingness to use nonmedical drugs for performance enhancement purposes. By using Structural Equation Models, we found that job demands (such as overtime and emotional demands) and a scarcity of resources (such as emotional stability) increased strain, consequently directly and indirectly increasing the willingness to use prescription drugs for cognitive enhancement. Moreover, emotional stability reduced the effect of certain demands on strain. These results delivered new insights into mechanisms behind nonmedical prescription drug use that can be used to prevent such behaviour and potential negative health consequences.
Will neuroscientists soon be able to read minds thanks to brain imaging techniques? We cannot answer this question without knowing the state of the art in neuroimaging. But neither can we answer this question without having some understanding of the concept to which the term "mind reading" refers. This article is an attempt to develop such an understanding. Our analysis takes place in two stages. In the first stage, we provide a categorical explanation of mindreading. The categorical explanation formulates empirical conditions that must be met for mindreading to be possible. In the second phase, we develop a benchmark for assessing the performance of mindreading experiments. The resulting conceptualization of mindreading helps to reconcile folk psychological judgments about what mindreading must entail with the constraints imposed by empirical strategies for achieving it.

While the nonmedical use of prescription drugs to enhance cognitive performance (NMUPD-CE) has received increasing media attention and provoked ethical debates, the social drivers of misusing this health-related drug remain understudied. Therefore, this study examined how descriptive and injunctive norms as social influences affect decisions to engage in NMUPD-CE. We tested competing assumptions about whether moral acceptability and positive and negative outcome expectations mediate or moderate the social norms effects. We used data from a Germany-wide, web-based survey with a sample of adult nonusers who were recruited offline (N= 13,443). We found that 62.09% of the respondents indicated at least some willingness for NMUPD-CE. Positive associations occurred between this willingness and both social norms, high positive and low negative outcome expectations, as well as higher moral acceptability. Moral acceptability and positive outcome expectations partially mediated both social norm effects, while negative outcome expectations only partially mediated injunctive norms. Moreover, positive and negative outcome expectations also moderated both social norm effects. This study provides insights into the understanding of social influence in the context of substance misuse and beyond. It suggests that social norms operate via moral acceptability and outcome expectations, while outcome expectations also lead to differential effects of social norms.
Predicting brain age is a relatively new tool in neuromedicine and neuroscience. It is widely used in research and clinical practice as a marker for biological age, for the general health of the brain and as an indicator of various brain-related disorders. Its usefulness in all these tasks depends on detecting outliers and thus not correctly predicting chronological age. The indicative value of age prediction comes from the gap between the chronological age of a brain and the predicted age, the "Brain Age Gap" (BAG). This article shows how the clinical and scientific application of brain age prediction tacitly pathologizes the conditions it addresses. It is argued that the tacit nature of this transformation obscures the need for its explicit justification.
Introduction: Moral judgment is of critical importance in the work context because of its implicit or explicit omnipresence in a wide range of work-place practices. The moral aspects of actual behaviors, intentions, and consequences represent areas of deep preoccupation, as exemplified in current corporate social responsibility programs, yet there remain ongoing debates on the best understanding of how such aspects of morality (behaviors, intentions, and consequences) interact. The ADC Model of moral judgment integrates the theoretical insights of three major moral theories (virtue ethics, deontology, and consequentialism) into a single model, which explains how moral judgment occurs in parallel evaluation processes of three different components: the character of a person (Agent-component); their actions (Deed-component); and the consequences brought about in the situation (Consequences-component). The model offers the possibility of overcoming difficulties encountered by single or dual-component theories.
Methods: We designed a 2 × 2 × 2-between-subjects design vignette experiment with a Germany-wide sample of employed respondents (N = 1,349) to test this model.
Results: Results showed that the Deed-component affects willingness to cooperate in the work context, which is mediated via moral judgments. These effects also varied depending on the levels of the Agent- and Consequences-component.
Discussion: Thereby, the results exemplify the usefulness of the ADC Model in the work context by showing how the distinct components of morality affect moral judgment.
The rise of neurotechnologies, especially in combination with artificial intelligence (AI)-based methods for brain data analytics, has given rise to concerns around the protection of mental privacy, mental integrity and cognitive liberty – often framed as “neurorights” in ethical, legal, and policy discussions. Several states are now looking at including neurorights into their constitutional legal frameworks, and international institutions and organizations, such as UNESCO and the Council of Europe, are taking an active interest in developing international policy and governance guidelines on this issue. However, in many discussions of neurorights the philosophical assumptions, ethical frames of reference and legal interpretation are either not made explicit or conflict with each other. The aim of this multidisciplinary work is to provide conceptual, ethical, and legal foundations that allow for facilitating a common minimalist conceptual understanding of mental privacy, mental integrity, and cognitive liberty to facilitate scholarly, legal, and policy discussions.

This study contributes to the emerging literature on public perceptions of neurotechnological devices (NTDs) in their medical and non-medical applications, depending on their invasiveness, framing effects, and interindividual differences related to personal needs and values. We conducted two web-based between-subject experiments (2×2×2) using a representative, nation-wide sample of the adult population in Germany. Using vignettes describing how two NTDs, brain stimulation devices (BSDs; NExperiment 1 = 1,090) and brain-computer interfaces (BCIs; NExperiment 2 = 1,089), function, we randomly varied the purpose (treatment vs. enhancement) and invasiveness (noninvasive vs. invasive) of the NTD, and assessed framing effects (variable order of assessing moral acceptability first vs. willingness to use first). We found a moderate moral acceptance and willingness to use BSDs and BCIs. Respondents preferred treatment over enhancement purposes and noninvasive over invasive devices. We also found a framing effect and explored the role of personal characteristics as indicators of personal needs and values (e.g., stress, religiosity, and gender). Our results suggest that the future demand for BSDs or BCIs may depend on the purpose, invasiveness, and personal needs and values. These insights can inform technology developers about the public’s needs and concerns, and enrich legal and ethical debates.
Researchers in applied ethics, and particularly in some areas of bioethics, aim to develop concrete and appropriate recommendations for action in morally relevant situations in the real world. However, in moving from more abstract levels of ethical reasoning to such concrete recommendations, it seems possible to develop divergent or even contradictory recommendations for action in a given situation, even in relation to the same normative principle or norm. This may give the impression that such recommendations are arbitrary and thus not well founded. Against this background, we first want to show that ethical recommendations for action, while contingent to some extent, are not arbitrary if they are developed in an appropriate way. To this end, we examine two types of contingencies that arise in applied ethical reasoning using recent examples of recommendations for action in the context of the COVID-19 pandemic. In doing so, we refer to a three-stage model of ethical reasoning for recommendations for action. However, this leaves open the question of how applied ethics can deal with contingent recommendations for action. Therefore, in a second step, we analyze the role of bridging principles for the development of ethically appropriate recommendations for action, i.e., principles that combine normative claims with relevant empirical information to justify certain recommendations for action in a given morally relevant situation. Finally, we discuss some implications for reasoning and reporting in empirically informed ethics.
This study examines how work stress affects the misuse of prescription drugs to augment mental performance without medical necessity (i.e., cognitive enhancement). Based on the effort–reward imbalance model, it can be assumed that a misalignment of effort exerted and rewards received increases prescription drug misuse, especially if employees overcommit. To test these assumptions, we conducted a prospective study using a nationwide web-based sample of the working population
in Germany (N = 11,197). Effort, reward, and overcommitment were measured at t1 and the 12 month frequency of prescription drug misuse for enhancing cognitive performance was measured at a one-year follow-up (t2). The results show that 2.6% of the respondents engaged in such drug misuse, of which 22.7% reported frequent misuse. While we found no overall association between misuse frequency and effort, reward, or their imbalance, overcommitment was significantly associated with
a higher misuse frequency. Moreover, at low levels of overcommitment, more effort and an effort–reward imbalance discouraged future prescription drug misuse, while higher overcommitment, more
effort, and an imbalance increased it. These findings suggest that a stressful work environment is a risk factor for health-endangering behavior, and thereby underlines the importance of identifying groups at risk of misusing drugs.
Researchers in applied ethics, and particularly in some areas of bioethics, aim to develop concrete and appropriate recommendations for action in morally relevant situations in the real world. However, in moving from more abstract levels of ethical reasoning to such concrete recommendations, it seems possible to develop divergent or even contradictory recommendations for action in a given situation, even in relation to the same normative principle or norm. This may give the impression that such recommendations are arbitrary and thus not well founded. Against this background, we first want to show that ethical recommendations for action, while contingent to some extent, are not arbitrary if they are developed in an appropriate way. To this end, we examine two types of contingencies that arise in applied ethical reasoning using recent examples of recommendations for action in the context of the COVID-19 pandemic. In doing so, we refer to a three-stage model of ethical reasoning for recommendations for action. However, this leaves open the question of how applied ethics can deal with contingent recommendations for action. Therefore, in a second step, we analyze the role of bridging principles for the development of ethically appropriate recommendations for action, i.e., principles that combine normative claims with relevant empirical information to justify certain recommendations for action in a given morally relevant situation. Finally, we discuss some implications for reasoning and reporting in empirically informed ethics.

This article critically addresses the conceptualization of trust in the ethical discussion on artificial intelligence (AI) in the specific context of social robots in care. First, we attempt to define in which respect we can speak of ‘social’ robots and how their ‘social affordances’ affect the human propensity to trust in human–robot interaction. Against this background, we examine the use of the concept of ‘trust’ and ‘trustworthiness’ with respect to the guidelines and recommendations of the High-Level Expert Group on AI of the European Union.

In the context of rapid digitalisation and the emergence of consumer health technologies, neurotechnological devices are associated with further hopes, but also with major ethical and legal concerns.

Machine learning (ML) is increasingly used to predict clinical deterioration in intensive care unit (ICU) patients through scoring systems. Although promising, such algorithms often overfit their training cohort and perform worse at new hospitals. Thus, external validation is a critical – but frequently overlooked – step to establish the reliability of predicted risk scores to translate them into clinical practice. We systematically reviewed how regularly external validation of ML-based risk scores is performed and how their performance changed in external data.
This article is a preprint and has not been peer-reviewed. It reports new medical research that has yet to be evaluated and so should not be used to guide clinical practice.
Artificial intelligence (AI) applications are finding their way into our everyday lives. In the field of medicine, this involves the optimisation of diagnosis and therapy, the use of health apps of all kinds, the provision of personalised medicine tools, the possibilities of robot-assisted surgery, optimised hospital data management and the development and provision of intelligent medical products. But are these constellations actually examples of artificial intelligence? What does ‘intelligence’ mean and what conditions must be met in order to be able to speak of ‘intelligence’? These questions are answered very differently depending on the context and disciplinary anchoring, resulting in a wide-ranging and multi-faceted discourse. What is undisputed, however, is that the quality and quantity of the applications categorised as AI raise numerous legal, ethical, social and scientific questions that have yet to be comprehensively addressed and satisfactorily resolved. While the law usually lags behind practical developments when it comes to regulating technology, a paradigm shift is taking place in the field of AI: at the end of April 2021, the European Commission presented a draft ‘Regulation laying down harmonised rules on artificial intelligence (Artificial Intelligence Act) and amending certain Union acts’ 2 (hereinafter referred to as the ‘VO-E’). The following explanations present the regulatory approach on which this draft is based as well as the resulting central definitions, duties and mechanisms. In the interest of a holistic approach, ethical, medical-scientific and social considerations are also taken into account.
Probably nowhere are technology and people so close, so intimately and intimately intertwined as in the fields of medicine, therapy and care. Numerous ethical questions are therefore raised at the nexus of medicine and technology. This volume pursues the dual aim of illuminating the entanglements of medicine, technology and ethics from different disciplinary perspectives on the one hand and, on the other, taking a look at practice, at the realms of experience of people working in medicine and their interactions with technologies.
Introduction
Although machine learning classifiers have been frequently used to detect Alzheimer’s disease (AD) based on structural brain MRI data, potential bias with respect to sex and age has not yet been addressed. Here, we examine a state-of-the-art AD classifier for potential sex and age bias even in the case of balanced training data.
Methods
Based on an age- and sex-balanced cohort of 432 subjects (306 healthy controls, 126 subjects with AD) extracted from the ADNI data base, we trained a convolutional neural network to detect AD in MRI brain scans and performed ten different random training-validation-test splits to increase robustness of the results. Classifier decisions for single subjects were explained using layer-wise relevance propagation.
Results
The classifier performed significantly better for women (balanced accuracy ) than for men (). No significant differences were found in clinical AD scores, ruling out a disparity in disease severity as a cause for the performance difference. Analysis of the explanations revealed a larger variance in regional brain areas for male subjects compared to female subjects.
Discussion
The identified sex differences cannot be attributed to an imbalanced training dataset and therefore point to the importance of examining and reporting classifier performance across population subgroups to increase transparency and algorithmic fairness. Collecting more data especially among underrepresented subgroups and balancing the dataset are important but do not always guarantee a fair outcome.
Background:
Resources are increasingly spent on artificial intelligence (AI) solutions for medical applications aiming to improve diagnosis, treatment, and prevention of diseases. While the need for transparency and reduction of bias in data and algorithm development has been addressed in past studies, little is known about the knowledge and perception of bias among AI developers.
Objective:
This study’s objective was to survey AI specialists in health care to investigate developers’ perceptions of bias in AI algorithms for health care applications and their awareness and use of preventative measures.

Background: Accurate prediction of clinical outcomes in individual patients following acute stroke is vital for healthcare providers to optimize treatment strategies and plan further patient care. Here, we use advanced machine learning (ML) techniques to systematically compare the prediction of functional recovery, cognitive function, depression, and mortality of first-ever ischemic stroke patients and to identify the leading prognostic factors.
The use of artificial intelligence (AI), i.e. algorithmic systems that can solve complex problems independently, will foreseeably play an important role in clinical and nursing practice. In clinical practice, AI systems are already in use to support diagnostic and therapeutic decisions or to work prognostically. For several years now, systems for diagnostic support in radiology have been tested and discussed (Wu et al. 2020; McKinney et al. 2020). This is accompanied by the hope of faster, more efficient and more effective diagnoses and decisions as well as new therapy and prognosis options, especially in big data-based medicine (i.e. in medical areas that rely on the processing of large amounts of complex and unstructured data). In nursing practice, AI plays a role primarily in connection with the use of nursing robots such as Paro or Pepper, which are intended to independently animate people in need of care, communicate with them or take over certain nursing tasks (Bendel 2018).
These expectations are offset by a number of ethical concerns, for example regarding the possible effects of an increasing use of AI-based systems on the medical and nursing role or the doctor-patient relationship. In addition, questions of data protection are discussed as well as possible social implications. Another focus of the debate is the possible ethical implications of the lack of explainability or explicability of diagnoses, therapeutic decisions and prognoses by AI-based systems and their significance for patients or the interaction between humans and medical technology in general. With regard to the use of care robots, the focus of the debates is on the conditions under which such systems can be considered trustworthy or what an appropriate use for people in need of care might look like.
The expectations outlined regarding the use of AI-based systems in medicine and nursing, as well as in particular the associated ethical challenges, also raise a number of legal questions. Of particular importance are questions of civil liability and criminal responsibility in the context of the use of AI-based systems. Insofar as an applied ethical reflection of new technological developments must fundamentally also take into account the applicable legal framework and the gaps and challenges that arise therein, an examination of these questions also seems necessary with a view to ethical analysis.

Progress in neurotechnology and Artificial Intelligence (AI) provides unprecedented insights into the human brain. There are increasing possibilities to influence and measure brain activity. These developments raise multifaceted ethical and legal questions. The proponents of neurorights argue in favour of introducing new human rights to protect mental processes and brain data. This article discusses the necessity and advantages of introducing new human rights focusing on the proposed new human right to mental self-determination and the right to freedom of thought as enshrined in Art.18 International Covenant on Civil and Political Rights (ICCPR) and Art. 9 European Convention on Human Rights (ECHR). I argue that the right to freedom of thought can be coherently interpreted as providing comprehensive protection of mental processes and brain data, thus offering a normative basis regarding the use of neurotechnologies. Besides, I claim that an evolving interpretation of the right to freedom of thought is more convincing than introducing a new human right to mental self-determination.
Neuronal optogenetics is a technique to control the activity of neurons with light. This is achieved by artificial expression of light-sensitive ion channels in the target cells. By optogenetic methods, cells that ate naturally light-insensitive can be made photosensitive and addressable by illumination and precisely controllable in time and space. So far, optogenetics has primarily been a basic research tool to better understand the brain. However, initial studies are already investigating the possibility of using optogenetics in humans for future therapeutic approaches for neuronal based diseases such as Parkinson's disease, epilepsy, or to promote stroke recovery. In addition, optogenetic methods have already been successfully applied to a human in an experimental setting. Neuronal optogenetics also raises ethical and legal issues, e.g., in relation to animal experiments and its application in humans. Additional ethical and legal questions may arise when optogenetic methods are investigated on cerebral organoids. Thus, for the successful translation of optogenetics from basic research to medical practice, the ethical and legal questions of this technology must also be answered, because open ethical and legal questions can hamper the translation. The paper provides an overview of the ethical and legal issues raised by neuronal optogenetics. In addition, considering the technical prerequisites for translation, the paper shows consistent approaches to address these open questions. The paper also aims to support the interdisciplinary dialogue between scientists and physicians on the one hand, and ethicists and lawyers on the other, to enable an interdisciplinary coordinated realization of neuronal optogenetics.
The wide parameter space of non-invasive brain stimulation, including dose (e.g., duration, intensity (current density), number of repetitions), inclusion/exclusion (e.g., subject’s age), and homeostatic effects, administration of tasks before and during stimulation, and, most importantly, placebo or nocebo effects, have to be taken into account. The outcomes of stimulation are expected to depend on these parameters and should be strictly controlled. The consensus among experts is that low-intensity tES is safe as long as tested and accepted protocols (including, for example, dose, inclusion/exclusion) are followed and devices are used which follow established engineering risk-management procedures. Devices and protocols that allow stimulation outside these parameters cannot claim to be “safe” where they are applying stimulation beyond that examined in published studies that also investigated potential side effects.
Brain stimulation devices marketed for consumer use are distinct from medical devices because they do not make medical claims and are therefore not necessarily subject to the same level of regulation as medical devices (i.e., by government agencies tasked with regulating medical devices). Manufacturers must follow ethical and best practices in marketing tES stimulators, including not misleading users by referencing effects from human trials using devices and protocols not similar to theirs.
The increasing availability of brain data within and outside the biomedical field, combined with the application of artificial intelligence (AI) to brain data analysis, poses a challenge for ethics and governance. We highlight the particular ethical implications of brain data collection and processing and outline a multi-level governance framework. This framework aims to maximize the benefits of facilitating the collection and further processing of brain data for science and medicine while minimizing the risks and preventing harmful use. The framework consists of four primary areas for regulatory intervention: binding regulation, ethics and soft law, responsible innovation and human rights.
In the past decade, artificial intelligence (AI) has become a disruptive force around the world, offering enormous potential for innovation but also creating hazards and risks for individuals and the societies in which they live. This volume addresses the most pressing philosophical, ethical, legal, and societal challenges posed by AI. Contributors from different disciplines and sectors explore the foundational and normative aspects of responsible AI and provide a basis for a transdisciplinary approach to responsible AI. This work, which is designed to foster future discussions to develop proportional approaches to AI governance, will enable scholars, scientists, and other actors to identify normative frameworks for AI to allow societies, states, and the international community to unlock the potential for responsible innovation in this critical field. This book is also available as Open Access on Cambridge Core.
In this chapter, Philipp Kellmeyer discusses how to protect mental privacy and mental integrity in the interaction of AI-based neurotechnology from the perspective of philosophy, ethics, neuroscience, and psychology. The author argues that mental privacy and integrity are important anthropological goods that need to be protected from unjustified interferences. He then outlines the current scholarly discussion and policy initiatives about neurorights and takes the position that while existing human rights provide sufficient legal instruments, an approach is required that makes these rights actionable and justiciable to protect mental privacy and mental integrity, for example, by connecting fundamental rights to specific applied laws.

Currently, the epistemic quality of algorithms and their normative implications are particularly in focus. While general questions of justice have been addressed in this context, specific questions of epistemic (in)justice have so far been neglected. We aim to fill this gap by analyzing some potential implications of behaviorally intelligent neurotechnology (B-INT). We argue that B-INT has a number of epistemic features that carry the potential for certain epistemic problems, which in turn are likely to lead to instances of epistemic injustice. To substantiate this claim, we will first introduce and explain the terminology and technology behind B-INT. Second, we will present four fictional scenarios for the use of B-INT and highlight a number of epistemic problems that could arise. Third, we will discuss their relationship to the concept of epistemic justice and possible examples of this. Thus, we will highlight some important and morally relevant implications of the epistemic properties of INT

Neuroenhancement is about improving a person's mental characteristics, abilities and performance. The various techniques of neuroenhancement offer new possibilities for improvement, but also harbour significant dangers. Neuroenhancement, therefore, poses both comprehensive normative challenges for individuals and society as a whole. This status report provides a concise overview of the current neuroenhancement debate. The definition, techniques and purposes of neuroenhancement are discussed and arguments for and against its use are analysed on a individual, interpersonal and socio-political level.

Technological self-optimisation is currently talked about everywhere. It includes research into new possibilities with regard to cosmetic surgery, functional implantology, brain doping and extending lifespan. There are considerable social reservations about many of these technical means, which are often not legally available. In their ethical assessment, Jan-Hendrik Heinrichs and Markus Rüther argue in favour of a differentiated perspective: in their opinion, the reservations are not suitable for justifying social ostracism or even binding bans for everyone. Rather, the freedom to organise oneself has priority, but this does not mean that there do not have to be clear rules for some areas. However, because self-determination can only be free if it is informed, the authors argue in favour of regulations that are determined by extensive information obligations rather than prohibitions. From an individual perspective, a series of moral recommendations can also be formulated which, although they cannot be enforced, provide an ethical compass to guide us through the thicket of ethical debate.
Neuroimaging can be used to collect a wide range of information about processes in the human brain. This status report provides information on the basic principles and possible applications of neuroimaging techniques in the neurosciences, examines the relevant legal standards and regulations and discusses the ethical challenges that arise in relation to the use of imaging techniques in the context of medical treatment and clinical research as well as in the context of criminal law.
In particular, the risk-benefit balance, the autonomy of patients, the protection of their privacy and more general considerations of justice in clinical research are taken into account.
Explainability for artificial intelligence (AI) in medicine is a hotly debated topic. Our paper presents a review of the key arguments in favor and against explainability for AI-powered Clinical Decision Support System (CDSS) applied to a concrete use case, namely an AI-powered CDSS currently used in the emergency call setting to identify patients with life-threatening cardiac arrest. More specifically, we performed a normative analysis using socio-technical scenarios to provide a nuanced account of the role of explainability for CDSSs for the concrete use case, allowing for abstractions to a more general level. Our analysis focused on three layers: technical considerations, human factors, and the designated system role in decision-making. Our findings suggest that whether explainability can provide added value to CDSS depends on several key questions: technical feasibility, the level of validation in case of explainable algorithms, the characteristics of the context in which the system is implemented, the designated role in the decision-making process, and the key user group(s). Thus, each CDSS will require an individualized assessment of explainability needs and we provide an example of how such an assessment could look like in practice.

Will brain imaging technology soon enable neuroscientists to read minds? We cannot answer this question without some understanding of the state of the art in neuroimaging. But neither can we answer this question without some understanding of the concept invoked by the term “mind reading.” This article is an attempt to develop such understanding. Our analysis proceeds in two stages. In the first stage, we provide a categorical explication of mind reading. The categorical explication articulates empirical conditions that must be satisfied if mind reading is to be achieved. In the second stage, we develop a metric for judging the proficiency of mind reading experiments. The conception of mind reading that emerges helps to reconcile folk psychological judgments about what mind reading must involve with the constraints imposed by empirical strategies for achieving it.

In this paper, we address the question of whether AI should be used for suicide prevention on social media data. We focus on algorithms that can identify persons with suicidal ideation based on their postings on social media platforms and investigate whether private companies like Facebook are justified in using these. To find out if that is the case, we start with providing two examples for AI-based means of suicide prevention in social media. Subsequently, we frame suicide prevention as an issue of beneficence, develop two fictional cases to explore the scope of the principle of beneficence and apply the lessons learned to Facebook’s employment of AI for suicide prevention. We show that Facebook is neither acting under an obligation of beneficence nor acting meritoriously. This insight leads us to the general question of who is entitled to help. We conclude that private companies like Facebook can play an important role in suicide prevention, if they comply with specific rules which we derive from beneficence and autonomy as core principles of biomedical ethics. At the same time, public bodies have an obligation to create appropriate framework conditions for AI-based tools of suicide prevention. As an outlook we depict how cooperation between public and private institutions can make an important contribution to combating suicide and, in this way, put the principle of beneficence into practice.

In this paper, I examine whether the use of artificial intelligence (AI) and automated decision-making (ADM) aggravates issues of discrimination as has been argued by several authors. For this purpose, I first take up the lively philosophical debate on discrimination and present my own definition of the concept. Equipped with this account, I subsequently review some of the recent literature on the use AI/ADM and discrimination. I explain how my account of discrimination helps to understand that the general claim in view of the aggravation of discrimination is unwarranted. Finally, I argue that the use of AI/ADM can, in fact, increase issues of discrimination, but in a different way than most critics assume: it is due to its epistemic opacity that AI/ADM threatens to undermine our moral deliberation which is essential for reaching a common understanding of what should count as discrimination. As a consequence, it turns out that algorithms may actually help to detect hidden forms of discrimination.
Alcohol misuse during adolescence (AAM) has been associated with disruptive development of adolescent brains. In this longitudinal machine learning (ML) study, we could predict AAM significantly from brain structure (T1-weighted imaging and DTI) with accuracies of 73 -78% in the IMAGEN dataset (n∼1182). Our results not only show that structural differences in brain can predict AAM, but also suggests that such differences might precede AAM behavior in the data. We predicted 10 phenotypes of AAM at age 22 using brain MRI features at ages 14, 19, and 22. Binge drinking was found to be the most predictable phenotype. The most informative brain features were located in the ventricular CSF, and in white matter tracts of the corpus callosum, internal capsule, and brain stem. In the cortex, they were spread across the occipital, frontal, and temporal lobes and in the cingulate cortex. We also experimented with four different ML models and several confound control techniques. Support Vector Machine (SVM) with rbf kernel and Gradient Boosting consistently performed better than the linear models, linear SVM and Logistic Regression. Our study also demonstrates how the choice of the predicted phenotype, ML model, and confound correction technique are all crucial decisions in an explorative ML study analyzing psychiatric disorders with small effect sizes such as AAM.
Predicting relapse for individuals with psychotic disorders is not well established, especially after discontinuation of antipsychotic treatment. We aimed to identify general prognostic factors of relapse for all participants (irrespective of treatment continuation or discontinuation) and specific predictors of relapse for treatment discontinuation, using machine learning.

This vignette-based study examined the willingness to feign symptoms to obtain a prescription following an analysis on who might use prescription stimulants to enhance performance (N = 3,468). It experimentally manipulated three factors: the social disapproval of prescription stimulant use for enhancement purposes, the physicians’ diagnostic efforts, and the medical condition (attention-deficit/hyperactivity disorder and narcolepsy); respondent characteristics of self-control, personal morality, and self-efficacy were also measured. Our results showed that social disapproval of prescription drug use, a personal morality that disapproves of drug use, high self-control, and high self-efficacy were negatively associated with the willingness to use. Willingness increased especially in situations of social approval when there was a stronger personal approval of drug use, or surprisingly when physicians’ diagnostic efforts were higher. The feigning willingness was lower in situations of social disapproval and when personal morality disapproved of feigning. Thus, personal and situational characteristics are relevant to understand both behaviors.

Deep learning requires large labeled datasets that are difficult to gather in medical imaging due to data privacy issues and time-consuming manual labeling. Generative Adversarial Networks (GANs) can alleviate these challenges enabling synthesis of shareable data. While 2D GANs have been used to generate 2D images with their corresponding labels, they cannot capture the volumetric information of 3D medical imaging. 3D GANs are more suitable for this and have been used to generate 3D volumes but not their corresponding labels. One reason might be that synthesizing 3D volumes is challenging owing to computational limitations. In this work, we present 3D GANs for the generation of 3D medical image volumes with corresponding labels applying mixed precision to alleviate computational constraints.
We generated 3D Time-of-Flight Magnetic Resonance Angiography (TOF-MRA) patches with their corresponding brain blood vessel segmentation labels. We used four variants of 3D Wasserstein GAN (WGAN) with: 1) gradient penalty (GP), 2) GP with spectral normalization (SN), 3) SN with mixed precision (SN-MP), and 4) SN-MP with double filters per layer (c-SN-MP). The generated patches were quantitatively evaluated using the Fréchet Inception Distance (FID) and Precision and Recall of Distributions (PRD). Further, 3D U-Nets were trained with patch-label pairs from different WGAN models and their performance was compared to the performance of a benchmark U-Net trained on real data. The segmentation performance of all U-Net models was assessed using Dice Similarity Coefficient (DSC) and balanced Average Hausdorff Distance (bAVD) for a) all vessels, and b) intracranial vessels only.
Our results show that patches generated with WGAN models using mixed precision (SN-MP and c-SN-MP) yielded the lowest FID scores and the best PRD curves. Among the 3D U-Nets trained with synthetic patch-label pairs, c-SN-MP pairs achieved the highest DSC (0.841) and lowest bAVD (0.508) compared to the benchmark U-Net trained on real data (DSC 0.901; bAVD 0.294) for intracranial vessels.
In conclusion, our solution generates realistic 3D TOF-MRA patches and labels for brain vessel segmentation. We demonstrate the benefit of using mixed precision for computational efficiency resulting in the best-performing GAN-architecture. Our work paves the way towards sharing of labeled 3D medical data which would increase generalizability of deep learning models for clinical use.
Utilising science and technology to maximize human performance is often an essential feature of military activity. This can often be focused on mission success rather than just the welfare of the individuals involved. This tension has the potential to threaten the autonomy of soldiers and military physicians around the taking or administering of enhancement neurotechnologies (e.g., pills, neural implants, and neuroprostheses). The Hybrid Framework was proposed by academic researchers working in the U.S. context and comprises “rules” for military neuroenhancement (e.g., ensuring transparency and maintaining dignity of the warfighter). Integrating traditional bioethical perspectives with the unique requirements of the military environment, it has been referenced by military/government agencies tasked with writing official ethical frameworks. Our two-part investigation explored the ethical dimensions of military neuroenhancements with military officers – those most likely to be making decisions in this area in the future. In three workshops, structured around the Hybrid Framework, we explored what they thought about the ethical issues of enhancement neurotechnologies. From these findings, we conducted a survey (N = 332) to probe the extent of rule endorsement. Results show high levels of endorsement for a warfighter’s decision-making autonomy, but lower support for the view that enhanced warfighters would pose a danger to society after service. By examining the endorsement of concrete decision-making guidelines, we provide an overview of how military officers might, in practice, resolve tensions between competing values or higher-level principles. Our results suggest that the military context demands a recontextualisation of the relationship between military and civilian ethics.
In the present article we examine the anthropological implications of “intelligent” neurotechnologies (INTs). For this purpose, we first give an introduction to current developments of INTs by specifying their central characteristics. We then present and discuss traditional anthropological concepts such as the “homo faber,” the concept of humans as “deficient beings,” and the concept of the “cyborg,” questioning their descriptive relevance regarding current neurotechnological applications. To this end, we relate these anthropological concepts to the characteristics of INTs elaborated before. As we show, the explanatory validity of the anthropological concepts analyzed in this article vary significantly. While the concept of the homo faber, for instance, is not capable of adequately describing the anthropological implications of new INTs, the cyborg proves to be capable of grasping several aspects of today’s neurotechnologies. Nevertheless, alternative explanatory models are needed in order to capture the new characteristics of INTs in their full complexity.
Over the last two decades, researchers have promised “neuroprosthetics” for use in physical rehabilitation and to treat patients with paralysis. Fulfilling this promise is not merely a technical challenge but is accompanied by consequential practical, ethical, and social implications that warrant sociological investigation and careful deliberation. In response, this paper explores how rehabilitation professionals evaluate the development and application of BCIs. It thereby also asks how the BCIs come to be seen as desirable or not, and implicitly, what types of persons, rights, and responsibilities are assumed in this discourse. To this end, we conducted a web-based survey (N=135) and follow-up interviews (N=15) with Canadian professionals in physical therapy, occupational therapy, and speech-language pathology. We find that rehabilitation professionals, like other publics, express hope and enthusiasm regarding the use of BCIs for assistive purposes. They envision BCI devices as powerful means to reintegrate patients and disabled people into social life but also express practical and ethical reservations about the technology, positioning themselves as uniquely qualified to inform responsible BCI design and implementation. These results further illustrate the nascent “co-production” of neural technologies and social order. More immediately, they also pose a serious challenge for implementing frameworks of responsible innovation; merely prescribing more inclusive technology development may not counteract technocratic processes and widely held ableist views about the need to augment certain bodies using technology.

An essential component of human-machine interaction (HMI) is the information exchanged between humans and machines to achieve specific effects in the world or in the interacting machines and/or humans. However, such information exchange in HMI may also shape the beliefs, norms and values of involved humans. Thus, ultimately, it may shape not only individual values, but also societal ones. This article describes some lines of development in HMI, where significant value changes are already emerging. For this purpose, we introduce the general notion of eValuation, which serves as a starting point for elaborating three specific forms of value change, namely deValuation, reValuation and xValuation. We explain these along with examples of self-tracking practices and the use of social robots.
First evidence shows that some parents engage in the health-endangering practice of (mis-)using prescription drugs to boost their children’s school performance. But little is known about parental perspectives on this phenomenon. This study aims to better understand parents’ perspectives on the non-medical use of prescription drugs to improve healthy children’s cognitive functioning. We conducted twelve semi-structured face-to-face interviews with a diverse sample of parents in Germany, and applied qualitative content analysis to explore their perspectives on instrumentalizing prescription drugs for improving the performance of healthy children, including their underlying knowledge (gaps), moral evaluations, evaluations of accompanied risks and benefits, opinions on potential motivators, and wishes regarding policy-making. The results show that parents typically believed themselves knowledgeable about such prescription drug (mis-)use, although they were not aware of anyone in their social environment taking them for enhancement. Parents generally considered such behavior to be morally reprehensible, cheating, and similar to doping in sports, and they typically claimed that no situation or occasion could motivate them to administer prescription drugs to their healthy children. Health risks (including side effects or addiction) were a typical expectation of drug use. That doctors should give such drugs to healthy young people was seen as unjustifiable. The results suggest that morality and risk–benefit evaluations of parents play a major role in their decision-making concerning this potentially risky instrumentalization of non-medical drugs. These insights are of distinct importance, especially for future research and further discussions on this topic, such as an evidence-based public dialog and ethics debates.

Follow us on LinkedIn, Instagram and YouTube to receive the latest information, exciting updates, and exclusive insights from the world of neuroethics.